When not diagnosed early and managed appropriately, common musculoskeletal injuries may result in long-term disabling conditions. Anterior cruciate ligament tears are some of the most common knee ligament injuries. Slipped capital femoral epiphysis may present with little or no hip pain, and subtle or absent physical and radiographic findings. Femoral neck stress fractures, if left untreated, may result in avascular necrosis, refractures and pseudoarthrosis. A delay in diagnosis of scaphoid fractures may cause early wrist arthrosis if nonunion results. Ulnar collateral ligament tears are a frequently overlooked injury in skiers. The diagnosis of Achilles tendon rupture is missed as often as 25 percent of the time. Posterior tibial tendon tears may result in fixed bony planus if diagnosis is delayed, necessitating hindfoot fusion rather than simple soft tissue repair. Family physicians should be familiar with the initial assessment of these conditions and, when appropriate, refer patients promptly to an orthopedic surgeon.
Musculoskeletal problems are frequently encountered by primary care physicians.1 Most of these problems get better with rest, ice and anti-inflammatory medication, and the more severe injuries are usually visible on radiograph. Unfortunately, certain musculoskeletal injuries are difficult to recognize for a variety of reasons and, when not diagnosed early, may develop into chronic disabling conditions. We discuss seven musculoskeletal injuries that require early diagnosis to ensure a good outcome.
Anterior Cruciate Ligament Tear
The anterior cruciate ligament is the most commonly injured ligament in the knee.2 A tear in this ligament usually occurs following a sudden valgus impact. Knees that are unstable as a result of anterior cruciate ligament tears put patients at risk for early degenerative joint disease, as well as subsequent damage to other structures of the knee.
Lachman's test (Figure 1) has been shown to be the most sensitive test for diagnosis of an anterior cruciate ligament tear. This test is often difficult to perform, in part because an acutely swollen and painful knee interferes with the patient's ability to relax. Patients with large knees and physicians with small hands can further compromise the examination. Often, by taking a good history, emphasizing the points below, the physician is able to determine the probability of an anterior cruciate ligament tear without the necessity of performing a Lachman's test.
FIGURE 1.

Lachman's test of the right knee. The examiner used the right hand to place anterior force on the lower leg while simultaneously using the left hand to place posterior force on the distal thigh. A good end point should be felt. Hands are reversed to test the left knee.
Eighty-five percent of patients who have an anterior cruciate ligament tear are immediately disabled and are not able to continue their activity.2 Patients often describe a feeling of “giving way” and report hearing or feeling a “pop” at the time of injury. If the knee swells within the first 24 hours, the swelling is most likely due to hemarthrosis rather than inflammation.3 Seventy percent of episodes of acute knee hemarthrosis are the result of anterior cruciate ligament tears.2,3 Two other conditions that cause hemarthrosis are patellar subluxation (kneecap slides out of place) and fracture within the knee. Table 1 summarizes conditions that make a tear in the anterior cruciate ligament a more likely diagnosis.
TABLE 1 Symptoms That Suggest a Tear in the Anterior Cruciate Ligament
| Knee swelling within 24 hours (hemarthrosis) |
| Hemarthrosis, patellar subluxation and fracture ruled out |
| Patient felt or heard a “pop” |
| Patient was unable to continue activity immediately after injury |
| Patient has a feeling that the knee “gives way” or is unstable |
Until magnetic resonance imaging (MRI) of the knee becomes more accurate or less expensive, referring the patient to an examiner experienced in the diagnosis of anterior cruciate ligament tear may be preferable to an MRI examination. This hypothesis is supported by three recent studies,4–6 all of which came to a similar conclusion: clinical assessment by a skilled examiner is at least similar to, if not more sensitive and specific than, an MRI in the diagnosis of an anterior cruciate ligament tear. The studies also concluded that MRI is not a cost-efficient test and adds little to the overall treatment program.
Surgery is the best option for athletes with an anterior cruciate ligament tear who want to continue activities requiring twisting or rapid changes in direction. In nonathletes or older patients, the decision should be based on the patient's activity level and expectations regarding activities. In these patients, alteration of lifestyle and use of a support or brace may represent a preferred alternative.
Slipped Capital Femoral Epiphysis
Slipped capital femoral epiphysis is the most common nontraumatic hip problem in adolescents.7 The diagnosis is often delayed, resulting in progression of the slip. The delay may be the result of late presentation to the physician or of misdiagnosis by the physician, because patients with slipped capital femoral epiphysis may present with little or no hip pain, and initial physical and radiographic findings may be subtle or absent.8
The stereotypical patient presenting with this lesion is a white obese boy, but this model is by no means universal. In a study9 of 1,630 children with slipped capital femoral epiphysis, 41 percent were girls and 58 percent were boys. Forty-seven percent were white and 25 percent were black. In 63 percent of the children, the child's weight was in or over the 90th percentile.
Slipped capital femoral epiphysis should be suspected in the child with a history of hip, groin, thigh or knee pain who walks with a limp. Pain upon internal rotation of the femur, causing decreased range of motion, is a key part of the physical examination. There may also be pain with hip abduction and flexion.
Radiographic examination involves drawing a line (Klein's line) along the superior femoral neck on the anteroposterior view (Figure 2a). Normally, a portion of the femoral head is above this line. In patients with slipped capital femoral epiphysis, the femoral head is below this line or a smaller portion of the femoral head is above this line compared with the contralateral view. The slip may be more noticeable on the frog-leg lateral view (Figure 2b).Some changes are very subtle, with only widening or blurring of the growth plate (Bloomberg's sign) showing.8 It is helpful to instruct the radiologist ahead of time that slipped capital femoral epiphysis is suspected. Patients with slipped capital femoral epiphysis should be referred urgently to an orthopedic surgeon for pinning to prevent progression of the slip and resultant long-term disability.
FIGURE 2A.

Anteroposterior view showing femoral head medially deviated in a patient with slipped capital femoral epiphysis.
FIGURE 2B.

Lateral view of femoral head. Note posterior deviation of 2 degrees.
Femoral Neck Stress Fractures
In a study10 of 23 patients with missed femoral neck stress fractures, the mean time to diagnosis was 14 weeks. Major complications included avascular necrosis, refractures and pseudoarthrosis. The authors speculate that early diagnosis would improve the prognosis.
A high index of suspicion is required to make a diagnosis of femoral neck stress fractures, since patients may present with only vague hip, groin or knee pain. A history of long-distance running or a sudden increase in activity should increase suspicion of femoral neck stress fracture. As with slipped capital femoral epiphysis, pain occurs with external or internal rotation of the hip. A stress fracture may not show up on radiographs for weeks (Figure 3a, 3b and 3c). If a femoral neck stress fracture is suspected but radiographs are not diagnostic, a bone scan should be performed. Unless the physician is well experienced with the treatment of femoral neck fractures, referral is indicated to prevent the complications described above.
FIGURE 3A.

Radiograph of right hip, initially read as negative for fracture.
FIGURE 3B.
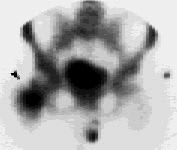
Bone scan of the patient in Figure 3a (arrow), showing increased uptake in right femoral neck characteristic of a stress fracture.
FIGURE 3C

Radiograph of the same patient, taken two months after the initial radiograph, showing callus formation (arrow).
Scaphoid Fracture
Scaphoid fracture is the most common fracture of the carpal bones.11,12 A fracture in the proximal or middle part of the scaphoid has an increased chance of nonunion because of the poor blood supply to these areas. A delay in diagnosis of one to two weeks increases the risk for nonunion.11 Nonunion of a scaphoid fracture can lead to early wrist arthrosis and can be avoided by either early casting or surgery.13
The typical history is distal radial wrist pain after a fall on the outstretched hand. If untreated, the pain gets better, then gets worse again.13 The classic physical finding is tenderness in the anatomic snuff box (Figure 4). Radiographs of the wrist should include a scaphoid view (Figure 5) that is anteroposterior with 30 degrees supination and ulnar deviation.
FIGURE 4.

Anatomic snuffbox, bordered medially by the tendon of the extensor pollicis longus, and laterally by the tendons of the extensor pollicis brevis and the abductor pollicis longus.
FIGURE 5.

Radiograph showing fracture of the scaphoid (arrow).
If radiographs are negative for fracture but a fracture is suspected clinically, the patient should be placed in a thumb spica splint. Clinical symptoms and radiographs are then rechecked in one to two weeks. 11,12 If radiographs are still negative and clinical suspicion of fracture is still high, a bone scan is the next step. If the scan is positive, the patient is placed in a thumb spica cast for six weeks longer.
Nondisplaced distal fractures are treated with thumb spica casting for six to eight weeks, with follow-up radiographs at three, six and 12 months.12 Reasons to refer a patient with scaphoid fracture are listed in Table 2.
TABLE 2 Reasons to Refer Patients with Scaphoid Fracture
| Fracture of proximal (or waist of the) scaphoid |
| Displacement greater than 2 mm |
| Carpal instability or dislocation present |
| Nonunion present |
| Family physician is uncomfortable with the 5 percent chance of nonunion |
Ulnar Collateral Ligament Tear (Gamekeeper's Thumb, Skier's Thumb)
Ulnar collateral ligament tear represents 60 percent of upper limb problems in skiers and is frequently overlooked and underdiagnosed.14 It is important to diagnose complete tears early because results of early surgical repair (within two to three weeks of the injury) are superior to results of late repair.15 Untreated tears can cause disabling instability of the hand, since the ulnar collateral ligament stabilizes the first metacarpophalangeal joint when the thumb is adducted against the index and middle fingers when gripping objects.
The typical history is of a sudden, forceful abduction of the thumb, such as during a fall on a skier's pole. Stress testing is performed by stabilizing the metacarpophalangeal joint in flexion and radially deviating the thumb (Figure 6). More than 30 degrees' deviation or more than 20 degrees' deviation compared with the opposite side suggests significant damage to the ulnar collateral ligament.16
FIGURE 6.
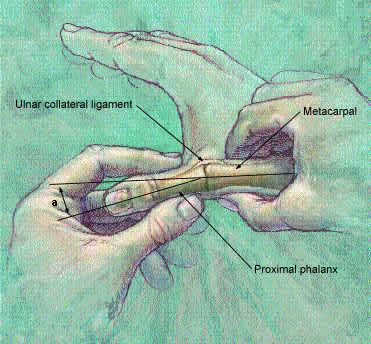
Stress test for ulnar collateral ligament tear. An end point is felt when the thumb is first flexed, then radially deviated, and the angle (a) between the first metacarpal and the proximal phalanx is assessed.
ILLUSTRATION BY SCOT BODELL
Ideally, radiographs should be taken before stress testing because, if an avulsion fracture is present, stress testing may further displace it. Stress radiographs (stress tests performed under x-ray) can help assess the degree of deviation but are not definitive.
When the torn ends of the ulnar collateral ligament cannot heal because the adductor aponeurosis interferes, the condition is called a Stener lesion. The disorder is difficult to diagnose on physical examination, but if it is suspected, referral to a hand surgeon is indicated. Other reasons to refer patients with this injury are given in Table 3.
TABLE 3 Reasons to Refer a Patient with Ulnar Collateral Ligament Tear
| No end point felt on stress testing |
| Deviation of 30 degrees on stress testing |
| Deviation of more than 20 degrees compared with the other side |
| Displaced avulsion fracture |
| Stener lesion |
A partial strain that does not require referral can be treated with either a thumb spica cast or a gamekeeper's thumb splint for four to six weeks. Active range of motion exercise is started at three to four weeks, with gradual return to full activity.
Achilles Tendon Rupture
The Achilles tendon is the second most frequently ruptured tendon, and the diagnosis is missed as often as 25 percent of the time.17,18 A partial rupture can be missed easily because, after the initial tear, the patient may have minimal pain and reasonably good plantar flexion strength. Therefore, the physician must have a high index of suspicion to make the diagnosis.
Classically, the patient notes a “pop” at the back of the heel and may report that it “felt like being kicked” in the heel. A patient with a complete tear will have an abnormal Thompson's test. This test is performed with the patient lying prone; an abnormal test is identified in the absence of plantarflexion of the foot with a hard squeeze of the calf. The patient with a partial tear has a normal Thompson's test but characteristically has a palpable defect. Following a complete rupture, the patient may have increased ankle dorsiflexion as a result of lack of tenodesis.
Surgery is usually the treatment of choice. Delayed primary repair is an option for the missed rupture,19 but results are better if surgery is done at an early stage. Conservative treatment with a cast is an option but has a higher re-rupture rate and the patient has decreased strength over long-term follow-up.17
Posterior Tibial Tendon Rupture
Although rupture of the posterior tibial tendon is relatively rare, we think it deserves a brief discussion here because primary care physicians frequently evaluate ankle sprains, and rupture of the posterior tibial tendon is frequently missed.20,21 Delayed diagnosis can cause fixed bony planus and necessitate difficult hindfoot fusion rather than simple soft tissue repair.
Rupture of the posterior tibial tendon should be strongly suspected in the adult patient who presents with a history of a twisting ankle injury, especially in the setting of a high-impact load, and generalized swelling and pain over the medial ankle. This injury occurs with increased frequency in the geriatric population, where it may not be readily suspected. Since the posterior tibial tendon helps maintain the arch of the foot (Figure 7), asymmetric pes planus (flat foot of the injured side) is suspicious for a rupture. The posterior tibial tendon also contributes to internal rotation of the foot and walking on toes; therefore, these motions should be checked on examination. MRI may help the physician make the diagnosis, and early surgical referral is indicated if a tear is found.
FIGURE 7.
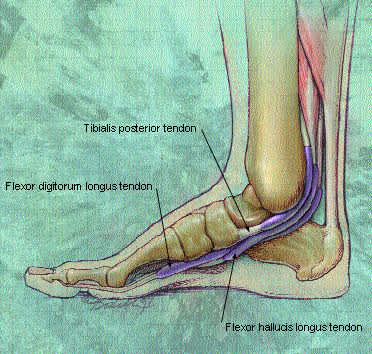
Drawing of posterior tibial tendon.
ILLUSTRATION BY SCOT BODELL
Table 4 reviews the diagnosis and treatment of commonly missed orthopedic injuries.
TABLE 4 Diagnosis and Treatment of Commonly Missed Orthopedic Injuries
| Injury | Diagnosis | Preferred treatment |
|---|---|---|
| Anterior cruciate ligament tear | Positive Lachman's test | Elective surgery |
| Slipped capital femoral epiphysis | Pain on internal hip rotation | Surgery as soon as practical |
| Femoral neck stress fracture | Bone scan | Rest, close follow-up* |
| Scaphoid fracture | Wrist pain, tenderness in anatomic “snuff box” | Thumb spica cast for 4 to 6 weeks* |
| Ulnar collateral ligament tear | Stress test shows >30 degrees of deviation in MCP joint | Mild: splint or cast |
| Severe: surgery | ||
| Achilles tendon rupture | Positive Thompson test | Surgical repair; partial tears can be casted |
| Posterior tibial tendon rupture | Asymmetric pes planus; MRI | Referral for surgery |
MCP = metacarpophalangeal; MRI = magnetic resonance imaging.
*—Physicians inexperienced in treatment of this condition should consider referral.
