A 36-year-old man presented to his family physician with a large number of slightly yellowish, raised papular lesions, 1 to 3 mm in diameter, on the posterior forearms and the anterior aspects of both legs (Figure 1). He experienced no significant symptoms. A specific clinical diagnosis was not evident, and a biopsy was perfomed to ascertain the nature of the lesions.
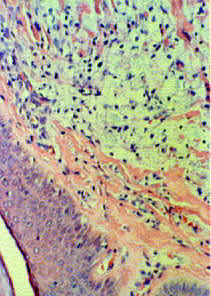
Figure 2 shows the raised bumps on the patient's left posterior forearm. The lesions were diagnosed as histiocytoma, which is seen in Figure 3 at 400 power magnification. The patient was not treated but, shortly thereafter, was admitted because of an episode of acute pancreatitis.


Question
Which one of the following is the correct diagnosis, given the patient's history and the physical appearance of the lesions?
A. Keratosis pilaris.
B. Histiocytoma.
C. Molluscum contagiosum.
D. Steroid-induced acne.
E. Type V hyperlipidemia with eruptive xanthomas.
Discussion
The answer is E: type V hyperlipidemia with eruptive xanthomas. Xanthomas are lipid-filled accumulations classically found on the extensor surfaces, as was noted on this patient. They are not necessarily associated with tendons. These lesions can be seen on skin biopsy as areas of fat-rich, foamy histiocytes, hence the original impression of a histiocytoma. The correct histologic diagnosis is “cutaneous xanthomas,” which is comparable to palpebral xanthelasma, a lesion of similar etiology.
The patient was admitted to the hospital for acute pancreatitis secondary to marked elevated serum triglyceride levels. This is not an uncommon finding associated with type V hyperlipidemia (familial lipase deficiency syndrome).
Keratosis pilaris is a variant form of atopic dermatitis. Plugs of desquamated skin partially block the small hair follicles, causing inflammation and sterile pustules outside the follicle. This results in yellowish raised mounds around the hairs, particularly on the arms, legs and trunk, but not in the classic acne-prone areas.
Molluscum contagiosum is a viral “wart” with small, pearly, umbilicated dome-shaped papules. They often occur in crops but would show classic molluscum bodies on biopsy. Steroid-induced acne would look like severe acne and would occur mostly on the face, the upper chest and the back, not on the extensor surfaces.
