
Am Fam Physician. 2000;61(4):1037-1042
See related patient information handout on Meckel's diverticulum, written by the authors of this article.
Although Meckel's diverticulum is the most prevalent congenital abnormality of the gastrointestinal tract, it is often difficult to diagnose. It may remain completely asymptomatic, or it may mimic such disorders as Crohn's disease, appendicitis and peptic ulcer disease. Ectopic tissue, found in approximately 50 percent of cases, consists of gastric tissue in 60 to 85 percent of cases and pancreatic tissue in 5 to 16 percent. The diagnosis of Meckel's diverticulum should be considered in patients with unexplained abdominal pain, nausea and vomiting, or intestinal bleeding. Major complications include bleeding, obstruction, intussusception, diverticulitis and perforation. The most useful method of diagnosis is with a technetium-99m pertechnetate scan, which is dependent on uptake of the isotope in heterotopic tissue. Management is by surgical resection.
Meckel's diverticulum is a true intestinal diverticulum that results from the failure of the vitelline duct to obliterate during the fifth week of fetal development.1,2 It contains all normal layers of the intestinal wall and, in approximately 50 percent of cases, contains tissue from other sites (ectopic tissue).2 This ectopic, or heterotopic, tissue can often be the cause of complications occurring in Meckel's diverticulum.
Meckel's diverticulum occurs in about 2 percent of the population, making it the most prevalent congenital abnormality of the gastrointestinal tract. Even so, it can be difficult to diagnose.2 It can be asymptomatic or mimic common abdominal disorders such as Crohn's disease, appendicitis and peptic ulcer disease.2 Many primary care physicians have never seen a patient with this abnormality, and the management involves a sometimes controversial decision about whether to surgically remove an incidentally discovered Meckel's diverticulum.
Illustrative Case
A 60-year-old woman presented to the emergency department with a complaint of nonradiating, waxing and waning epigastric abdominal pain of two to three hours' duration, with associated nausea and anorexia. There was no history of fever, diarrhea, constipation, melena, hematochezia or urinary symptoms.
The patient had been evaluated and treated for abdominal complaints in the past. She had undergone a total abdominal hysterectomy and bilateral salpingo-oophorectomy for cervical stenosis and pelvic pain with incidental appendectomy one year before and a cholecystectomy several years earlier. Abdominal ultrasounds, multiple upper gastrointestinal studies and an air contrast barium enema had been normal since the cholecystectomy. These examinations were performed because of continued complaints of nonspecific abdominal pain.
The patient's physical examination was non-specific. She was afebrile and normotensive and had a normal pulse and respiration. Her abdomen had nonlocalized upper- to midabdominal tenderness with no guarding or rebound, no organ enlargement or masses, and positive bowel sounds. The rectal examination was normal, with guaiacnegative stool. Her complete blood cell count was normal with a white blood cell count of approximately 9,000 per mm3 (9 × 109 per L). Electrolytes, liver function, urinalysis and amylase levels were all normal. The chest radiograph was clear, and the flat and upright abdominal films were normal, without air-fluid level, dilation or free air.
The patient was admitted to the hospital with intractable abdominal pain. She was given nothing by mouth and was placed on maintenance intravenous fluids. The next day, examination revealed right lower quadrant tenderness with slight guarding and rebound, which was confirmed on pelvic examination. The patient's stool was still guaiac-negative. However, her temperature had climbed to 37.5°C (99.6°F), and her white blood cell count had fallen to 5,000 per mm3 (5 × 109 per L) with a left shift. Hemoglobin and hematocrit levels, as well as electrolytes, blood urea nitrogen and creatinine levels, remained normal.
During her previous abdominal surgery, an incidentally discovered wide-mouthed, relatively short Meckel's diverticulum had been noted. The physician had determined that it was asymptomatic and elected to leave the diverticulum in place. In light of the patient's current condition, surgery was recommended for suspected Meckel's diverticulum.
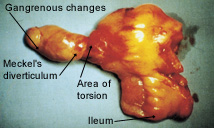
At laparotomy, an axially torsed, gangrenous Meckel's diverticulum was found without ileal volvulus. The lead point for the torsion was a fibrous adhesion attached between the distal tip of the diverticulum and the peritoneal surface. A diverticulectomy and segmental ileal resection were performed, and the patient had an uneventful postoperative course and recovery.
Incidence and Natural History
The incidence of Meckel's diverticulum in the general population has been estimated to be about 2 percent; reports from autopsy and retrospective studies range from 0.14 to 4.5 percent.1,3–6 Although Meckel's diverticulum occurs equally in both sexes,7–9 it causes complications more frequently in males1,9,10 and, therefore, is more often diagnosed in males.7 Early literature11,12 has quoted complication rates as high as 25 percent; however, results of a 15-year study set the risk of developing complications at 4.2 percent.13 This study of 202 patients did not include any cases of incidentally found diverticulum; it is the largest series of cases of complicated Meckel's diverticulum ever reported.
A population-based study10 from 1950 to 1992 found the incidence of a diverticular complication to be 87.4 per 100,000 person-years, translating to a 6.4 percent lifetime risk (lifetime = 80 years of age) of a person developing a complication related to the diverticulum. In this study,10 there was no decrease in the likelihood of complications with age. More recently, a 10-year retrospective study9 also reported an even age distribution in patients with complications. This issue of correlating age with the incidence of complications is not settled; therefore, age alone should not be the sole criterion for a decision to perform an incidental diverticulectomy.
Anatomy and Embryology
During early fetal development, the fetal midgut is attached to the yolk sac for nutrition via the omphalomesenteric duct (vitelline duct, or yolk stalk).1 If this duct does not involute by the seventh week of gestation, various developmental remnants may be left1 (Figure 1). Failure of the most proximal portion of the duct to obliterate results in a Meckel's diverticulum.14 The yolk sac is continuous with the embryo and contains all layers of the intestinal wall; therefore, the diverticulum that forms from the yolk stalk also contains all layers of the intestinal wall.15
In addition to the normal layers of the intestinal wall, approximately 50 percent of diverticula contain ectopic tissue.2 In surgical exploration, this ectopic tissue has been described as “strange granular tissue”; however, in one 15-year study, diagnosis by palpation at surgery led to 14 false-positive results.14 This overdiagnosis indicates that palpation at surgery is not a definitive indication of pathology.14
Meckel's diverticulum arises from the antimesenteric border—the part of the intestine that lies opposite the mesenteric attachment. Ninety percent of the diverticula are within 90 cm of the ileocecal valve, although reports of diverticula up to 180 cm from the ileocecal valve have occurred.7 Its blood supply comes from a terminal branch of the superior mesenteric artery that crosses the ileum to the diverticulum.1,7,16,17 Meckel's diverticulum typically presents as short and wide mouthed, as in the case study presented here.18 This shape often makes detection difficult.18,19
Pathologic Association or Conditions
Ectopic tissue (tissue existing in other than its original intended location) is found in up to 55 percent of Meckel's diverticula.20 Gastric and pancreatic tissue predominate, with corresponding incidences of 60 to 85 percent and 5 to 16 percent.1,10,16 The highly acidic secretions of gastric tissue may cause ulcerations that often lead to early diagnosis because of symptoms of gastrointestinal bleeding.7 The alkaline secretions of ectopic pancreatic tissue can also cause ulcerations.14 Reports have cited other tissues such as colonic, duodenal, jejunal, hepatic and endometrial; however, these occurrences are quite rare and are not in reports of complications.3,7,16
Malignancies may also occur but are found in only 0.5 to 4.9 percent of patients with complications of Meckel's diverticulum. Sarcomas are the most common neoplasm, followed by carcinoids and adenocarcinomas.3
Diagnosis
The diagnosis of symptomatic Meckel's diverticulum is difficult to make, especially in adults.7,11,21 The diagnosis must be considered in anyone with unexplained abdominal complaints, nausea and vomiting, or intestinal bleeding.22,23 Meckel's diverticulum can mimic a variety of more common ailments, such as peptic ulcer disease, gastroenteritis, biliary colic, colonic diverticulitis and milk allergy.7,16,20 Appendicitis is the most common preoperative diagnosis in cases of complicated Meckel's diverticulum.7 The illustrative case in this article reveals the nonspecific nature of the subjective and objective findings. Table 11 summarizes the characteristics of complications of Meckel's diverticulum from the findings of a chart review of 402 patients.
The diagnosis cannot be made with plain radiographs, and arteriography is not always diagnostic because arterial supply is not always abnormal.7 Contrast studies such as upper gastrointestinal series with small bowel follow-through are of limited value because the layers of barium-filled intestine will obstruct the view of the diverticulum.1 Computed tomographic scans are often nonspecific but occasionally helpful.24–26 The most useful method of detection of a Meckel's diverticulum is technetium-99m pertechnetate scanning. However, the technetium scan depends on uptake by heterotopic gastric mucosa.7,10,16,27
Not all diverticula contain ectopic tissue; because complications such as bleeding are often caused by ectopic gastric tissue, diagnosis may be assisted in symptomatic cases.3,11 In technetium-99m pertechnetate scanning, technetium-99m pertechnetate is injected intravenously; over time, it accumulates in the gastric mucosa.3
In children, the scan has a sensitivity of 85 percent and a specificity of 95 percent, but in adults, the sensitivity falls to 62.5 percent and specificity to only 9 percent.25,28 Many conditions can cause a false-positive diagnosis in adults: mucosal hyperemia of any cause, angiomas, urinary tract obstruction, an ectopic kidney or uterine pooling of blood.3 False-negative results are less common but causative conditions include impaired vascular supply, recent barium gastrointestinal study, premedication with atropine, a small diverticulum or hemorrhage washing out the isotope.3,16
The accuracy of the scan can be improved with the use of pentagastrin, which increases technetium uptake in gastric mucosa; however, it may also increase the washing away of the isotope by stimulating peristalsis.3,29 Cimetidine (Tagamet) improves diagnostic accuracy by inhibiting the intraluminal release of technetium, and glucagon does so as an antiperistaltic.3,29 A combination of pentagastrin and glucagon can be used to increase the uptake of the isotope and cease peristalsis simultaneously.26 When the Meckel's scan is nondiagnostic or in patients with nonbleeding presentations, ultrasonography is perhaps the most useful noninvasive method of achieving diagnosis.25
Management
The approach to treatment of a Meckel's diverticulum depends on whether it was discovered incidentally or as a result of symptoms. Ileal resection has traditionally been the treatment of choice for asymptomatic diverticulum, because the extent of heterotopic tissue and disease cannot be determined by palpation, and ulcerations can recur if the ectopic tissue persists.7 Ileal resection permits the removal of any damaged tissue, inflammation and ectopic tissue.7
Perhaps the most controversial area of management with regard to Meckel's diverticulum has been the asymptomatic patient with an incidentally discovered diverticulum. Strategies that have taken into account factors such as the age and sex of the patient, the length of the diverticulum and the diameter of the mouth or base of the diverticulum have proved to be ineffective in assisting the decision to prophylactically remove this congenital developmental variant.3,4,7,10,14
A physician can choose to leave the incidentally discovered diverticulum or perform a simple diverticulectomy or an ileal resection. Some physicians have voiced concern that ectopic tissue may be left behind if ileal resection is not performed; however, because the ectopic tissue is generally found at the distal end of the diverticulum, it will usually be included in the excised diverticulum.7 If the diverticulum is left intact, any fibrous bands attached to the diverticulum must be excised to prevent any future torsion or obstruction.7
Researchers involved in the previously mentioned 15-year retrospective chart review concluded that prophylactic diverticulectomy is unwarranted because the likelihood that an asymptomatic diverticulum will become symptomatic is low (about 4.2 percent), and that rate decreases with age.14 However, several factors now lend support to the concept of prophylactic diverticulectomy.
Another previously mentioned study10 did not support the theory that the incidence of complications from Meckel's diverticulum decreases with age. Once a Meckel's diverticulum develops complications and is surgically removed, the operative mortality, morbidity and cumulative long-term risk of postoperative complications are 2 percent, 12 percent and 7 percent, respectively.10 For Meckel's diverticula that are incidentally discovered and removed, the corresponding rates are 1 percent, 2 percent and 2 percent, respectively.10
Laparoscopy can be useful in the diagnosis and treatment of Meckel's diverticulum. In addition, the laparoscope can be used to remove an incidentally discovered diverticulum. The literature has also reported the successful use of laparoscopic diverticulectomy in infants with bleeding Meckel's diverticulum.19,30 Also, the now-proven safety and ease of the gastrointestinal stapling device have made this an acceptable tool in simple, uncomplicated diverticulectomy, provided the diverticulum fits easily in the device.3 In this technique, the mouth of the diverticulum is stapled before the diverticulum is removed; this allows the diverticulectomy to be performed without opening the bowel's lumen, which lowers the chances of contamination.31 Opponents of prophylactic diverticulectomy have addressed the morbidity and mortality that occur in resection of incidentally found diverticula; however, this concern does not reflect the ease and safety seen in these new techniques.32
Complications
As stated earlier, a person with Meckel's diverticulum has a 4 to 6 percent lifetime risk of developing a complication.10 The major complications are hemorrhage, obstruction, intussusception, diverticulitis and perforation.1,4,10,11,17 Bleeding is the most common complication occurring in children, and it typically presents as hematochezia.2 The hemorrhage is a result of heterotopic gastric mucosa leading to ulceration.3,11 Most adults present with obstruction, diverticulitis or both.3,11,14,21 Obstruction is often caused by fibrous bands attached to the diverticulum, as seen in the illustrative case.
This illustrative case demonstrates a rare phenomenon of axial torsion of the diverticulum, resulting in a compromised blood supply and gangrene. This condition could be considered a severe form of diverticulitis.32–34 Less frequently, fistulas can form in the presence of perforation, especially in association with Crohn's disease.3,35 However, there is not an increased incidence of Meckel's diverticulum in patients with Crohn's disease.3,35 A Meckel's diverticulum can also be part of the contents of a Littre's or diverticular hernia.3,7,16