to the editor: We read with interest the recent review article on endometriosis by Dr. Wellbery.1 We would like to add one additional comment about estrogen replacement therapy following hysterectomy and oophorectomy for symptomatic endometriosis.
We describe the case of a 68-year-old woman who underwent total abdominal hysterectomy and bilateral salpingooophorectomy in 1972 for intractable pelvic pain due to endometriosis. She was subsequently placed on estrogen-only replacement therapy. In November 1999, she presented to her primary care physician complaining of vaginal pressure and bleeding. A pelvic examination revealed a submucosal nodule at the vaginal apex, which was confirmed on pelvic ultrasonography as a 3 × 2.6-cm mass.
The patient subsequently underwent surgical resection with pelvic lymph node dissection. Pathologic examination of the vaginal mass revealed a moderately differentiated endometroid adenocarcinoma (see the accompanying figure). No associated foci of endometriosis were identified.
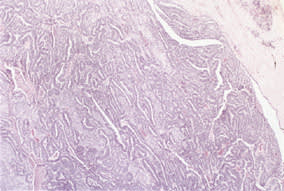
Endometroid adenocarcinoma. Low-power view of moderately differentiated endometroid adenocarcinoma of the vagina (40X).
The increased risk of developing intrauterine endometrial adenocarcinoma with prolonged unopposed estrogen therapy is well established. However, numerous investigators have reported endometrial malignancies arising in endometriotic foci following unopposed estrogen stimulation.2–4 Adenocarcinomas comprise the majority of these tumors, but stromal sarcomas also have been reported.5 Reported sites of malignancy include the vagina, rectum, cul-de-sac and rectovaginal septum.2
According to Sampson,6 who first described adenocarcinoma arising in endometriosis, histologic evidence of endometriosis in close proximity to a tumor should be identified before a definitive correlation between the two can be established. Although we did not see endometriosis in the current case, the patient's history and the site of the tumor were suggestive of an association.
Although unopposed estrogens are commonly administered to women who have undergone hysterectomies, physicians are urged to bear in mind the original indications for the procedure. If the hysterectomy was performed in the context of endometriosis, combined (estrogen and progesterone) hormone replacement therapy should be considered.
editor's note: This letter was sent to the author of “Diagnosis and Treatment of Endometriosis,” who declined to reply.
