Lipomas are adipose tumors that are often located in the subcutaneous tissues of the head, neck, shoulders, and back. Lipomas have been identified in all age groups but usually first appear between 40 and 60 years of age. These slow-growing, nearly always benign, tumors usually present as nonpainful, round, mobile masses with a characteristic soft, doughy feel. Rarely, lipomas can be associated with syndromes such as hereditary multiple lipomatosis, adiposis dolorosa, Gardner's syndrome, and Madelung's disease. There are also variants such as angiolipomas, neomorphic lipomas, spindle cell lipomas, and adenolipomas. Most lipomas are best left alone, but rapidly growing or painful lipomas can be treated with a variety of procedures ranging from steroid injections to excision of the tumor. Lipomas must be distinguished from liposarcoma, which can have a similar appearance.
Lipomas are slow-growing, nearly always benign, adipose tumors that are most often found in the subcutaneous tissues.1 Most lipomas are asymptomatic, can be diagnosed with clinical examination (Table 1) and do not require treatment. These tumors may also be found in deeper tissues such as the intermuscular septa, the abdominal organs, the oral cavity, the internal auditory canal, the cerebellopontine angle and the thorax.2–4 Lipomas have been identified in all age groups but usually first appear between 40 and 60 years of age.5 Congenital lipomas have been observed in children.6 Some lipomas are believed to have developed following blunt trauma.7
TABLE 1 Differential Diagnosis of Lipoma
| Epidermoid cyst |
| Subcutaneous tumors |
| Nodular fasciitis |
| Liposarcoma |
| Metastatic disease |
| Erythema nodosum |
| Nodular subcutaneous fat necrosis |
| Weber-Christian panniculitis |
| Vasculitic nodules |
| Rheumatic nodules |
| Sarcoidosis |
| Infections (e.g., onchocerciasis, loiasis) |
| Hematoma |
While solitary lipomas are more common in women, multiple tumors (referred to as lipomatosis) are more common in men.2,8 Hereditary multiple lipomatosis, an autosomal dominant condition also found most frequently in men, is characterized by widespread symmetric lipomas appearing most often over the extremities and trunk2,9 (Figure 1). Lipomatosis may also be associated with Gardner's syndrome, an autosomal dominant condition involving intestinal polyposis, cysts, and osteomas.8 The term Madelung's disease, or benign symmetric lipomatosis, refers to lipomatosis of the head, neck, shoulders, and proximal upper extremities. Persons with Madelung's disease, often men who consume alcohol, may present with the characteristic “horse collar” cervical appearance.2,10 Rarely, these patients experience swallowing difficulties, respiratory obstruction, and even sudden death.1,2
FIGURE 1.

Multiple lipomatosis of the trunk (hereditary multiple lipomatosis).
Evaluation
Lipomas usually present as nonpainful, round, mobile masses, with a characteristic soft, doughy feel. The overlying skin appears normal. Lipomas can usually be correctly diagnosed by their clinical appearance alone.
Microscopically, lipomas are composed of mature adipocytes arranged in lobules, many of which are surrounded by a fibrous capsule. Occasionally, a nonencapsulated lipoma infiltrates into muscle, in which case it is referred to as an infiltrating lipoma.5,11,12
Four other types of lipomas may be noted on a biopsy specimen. Angiolipomas are a variant form with co-existing vascular proliferation.2,11 Angiolipomas may be painful and usually arise shortly after puberty. Pleomorphic lipomas are another variant in which bizarre, multinucleated giant cells are admixed with normal adipocytes.1,13 Pleomorphic lipomas' presentation is similar to that of other lipomas, but they occur predominantly in men 50 to 70 years of age. A third variant, spindle cell lipomas, has slender spindle cells admixed in a localized portion of regular-appearing adipocytes.14,15 A newly described variant of superficial lipoma, adenolipoma, is characterized by the presence of eccrine sweat glands in the fatty tumor; this type is often located on the proximal parts of the limbs.1
A rare clinical consideration is Dercum's disease, or adiposis dolorosa, which is characterized by the presence of irregular painful lipomas most often found on the trunk, shoulders, arms, forearms, and legs.8 Dercum's disease is five times more common in women, is often found in middle age, and has asthenia and psychic disturbances as other prominent features.
Malignancy is rare but can be found in a lesion with the clinical appearance of a lipoma. Liposarcoma presents in a fashion similar to that of a lipoma and appears to be more common in the retroperitoneum, and on the shoulders and lower extremities.8 Some surgeons recommend complete excision of all clinical evidence of a lipoma to exclude a possible liposarcoma, especially in fast-growing lesions.8 Recently, magnetic resonance imaging has been used with some success to differentiate lipomas and liposarcomas.16,17
Treatment
NONEXCISIONAL TECHNIQUES
Nonexcisional treatment of lipomas, which is now common, includes steroid injections and liposuction.
Steroid injections result in local fat atrophy, thus shrinking (or, rarely, eliminating) the lipoma. Injections are best performed on lipomas less than 1 inch in diameter. A one-to-one mixture of 1 percent lidocaine (Xylocaine) and triamcinolone acetonide (Kenalog), in a dosage of 10 mg per mL, is injected into the center of the lesion; this procedure may be repeated several times at monthly intervals.8 The volume of steroid depends on the size of the lipoma, with an average of 1 to 3 mL of total volume administered. The number of injections depends on the response, which is expected to occur within three to four weeks. Complications, which are rare, are the result of the medication or the procedure, and can be prevented by injecting the smallest total amount possible and by positioning the needle so that it is in the center of the lipoma.
Liposuction can be used to remove small or large lipomatous growths, particularly those in locations where large scars should be avoided. Complete elimination of the growth is difficult to achieve with liposuction.8,18 Office procedures using a 16-gauge needle and a large syringe may be safer than large-cannula liposuction. Diluted lidocaine usually provides adequate anesthesia for office liposuction.
PREPARATION FOR EXCISION
Surgical excision of lipomas often results in a cure. Before the surgery, it is often helpful to draw an outline of the lipoma and a planned skin excision with a marker on the skin surface (Figure 2). The outline of the tumor often helps to delineate margins, which can be obscured after administration of the anesthetic. Excision of some skin helps to eliminate redundancy at closure.
FIGURE 2.

Proposed incision removing skin over the lipoma. The palpable borders of the lipoma are marked to aid the surgeon in complete removal.
The skin is then cleansed with povidone iodine (Betadine) or chlorhexidine (Betasept) solution, making sure to avoid wiping away the skin markings. The area is draped with sterile towels. Local anesthesia is administered with 1 or 2 percent lidocaine with epinephrine, usually as a field block. Infiltrating the anesthetic in the subcutaneous area surrounding the operative field creates a field block.
ENUCLEATION
Small lipomas can be removed by enucleation. A 3-mm to 4-mm incision is made over the lipoma. A curette is placed inside the wound and used to free the lipoma from the surrounding tissue. Once freed, the tumor is enucleated through the incision using the curette. Sutures generally are not needed, and a pressure dressing is applied to prevent hematoma formation.
EXCISION
Larger lipomas are best removed through incisions made in the skin overlying the lipoma. The incisions are configured like a fusiform excision following the skin tension lines and are smaller than the underlying tumor. The central island of skin to be excised is grasped with a hemostat, or Allis clamp, which is used to provide traction for the removal of the tumor (Figure 3). Dissection is then performed beneath the subcutaneous fat to the tumor. Any tissue cutting is performed under direct visualization using a no. 15 scalpel or scissors around the lipoma. Care must be taken to avoid nerves or blood vessels that may lie just beneath the tumor.
FIGURE 3.
The skin inside the incision grasped with a hemostat to provide traction. The lipoma is dissected from the surrounding tissue using scissors or a scalpel.
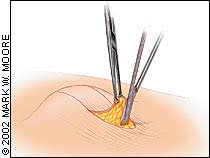
Once a portion of lipoma has been dissected from the surrounding tissue, hemostats or clamps can be attached to the tumor to provide traction for removal of the remainder of the growth. Once it is freed, the lipoma is delivered as a whole (Figure 4). The surrounding tissue in the hole can be palpated to ensure complete removal of the tumor. Table 2 lists possible complications of excision.
FIGURE 4.
Once freed, the lipoma is delivered as a whole, and hemostasis is achieved.
TABLE 2 Complications of Lipoma Excision
| Surgical infection/cellulitis/fasciitis |
| Ecchymosis |
| Hematoma formation |
| Injury to nearby nerves with permanent paresthesia/anesthesia |
| Injury to nearby vessels/vascular compromise |
| Permanent deformity secondary to removal of a large lesion |
| Excessive scarring with cosmetic deformity or contracture |
| Muscle injury/irritation |
| Fat embolus |
| Periostitis/osteomyelitis |
| Seroma |
Adequate hemostasis is achieved following the removal of the lipoma using hemostats or suture ligation. The dead space is closed beneath the skin using buried, interrupted 3-0 or 4-0 Vicryl sutures (Figure 5). Occasionally drains may have to be placed to prevent fluid accumulation, but this should be avoided if possible. The skin is then closed with interrupted 4-0 or 5-0 nylon sutures. A pressure dressing is placed to reduce the incidence of hematoma formation. The patient is given routine wound care instructions, and the wound is checked in two to seven days. The sutures are removed after seven to 21 days, depending on the body location. Specimens should be submitted for histologic analysis.
FIGURE 5.
Interrupted 3-0 or 4-0 Vicryl sutures are used to partially close the dead space.
