The formation of corns and calluses can be caused by mechanical stresses from faulty footgear (the wearing of poorly fitting shoes), abnormal foot mechanics (deformity of the foot exerting abnormal pressure), and high levels of activity. Corns and calluses result from hyperkeratosis, a normal physiologic response of the skin to chronic excessive pressure or friction. Treatment should provide symptomatic relief and alleviate the underlying mechanical cause. The lesions will usually disappear following the removal of the causative mechanical forces. Most lesions can be managed conservatively by the use of properly fitting shoes and padding to redistribute mechanical forces. Surgery is only indicated if conservative measures fail and should be aimed at correcting the abnormal mechanical stresses.
Trauma to the skin and soft tissue layers secondary to mechanical pressure and irritation are problems often overlooked by physicians; however, many of these mechanical injuries are very uncomfortable to the patient. Some of the most common mechanical injuries of the lower extremity present as corns and calluses. Symptoms may be severe enough to seriously affect a person's gait and choice of footgear or activities. Most corns and calluses will resolve with appropriate conservative treatment, making the proper diagnosis and treatment essential.1
Corns and calluses result from hyperkeratosis, which is caused by an increase in keratinocyte activity associated with stimulation of the epidermis from chronic pressure or friction on the skin. Examples include irritation from poorly fitting shoes or abnormal pressure caused by a deformity of the foot.2 [Evidence level C, consensus/expert opinion] Hyperkeratosis is a normal protective response of the skin, which becomes pathologic when the callus or corn grows so large that it becomes the source of symptoms.3
Corn
A corn is a circumscribed hyperkeratotic lesion with a central conical core of keratin that causes pain and inflammation. The conical core in a corn, which is a thickening of the stratum corneum, is a protective response to the mechanical trauma. This central core distinguishes the corn from the callus. Corns are divided into two subtypes: the hard corn (heloma durum) and the soft corn (heloma molle).
The hard corn, which is the most common type, appears as a dry, horny mass of hyperkeratosis with a hard central core. Hard corns most commonly occur on the dorsolateral aspect of the fifth toe (Figure 1) or the dorsum of the interphalangeal joints of the lesser toes.
FIGURE 1.

Hard corn on lateral aspect of fifth metatarsal.
The soft corn results from the absorption of an extreme amount of moisture from perspiration and is noted by its characteristic macerated appearance. The soft corn is an extremely painful lesion that can develop between any of the toes but most commonly develops between the fourth and fifth toes4 (Figure 2).
FIGURE 2.

Soft corn between fourth and fifth metatarsals.
A common cause of hard and soft corns is hammertoe deformity. Successful treatment depends on the severity of the hammertoe deformity. In young persons who have a fixed deformity, conservative measures will produce better results than surgery. Reducible deformities may respond to a crest pad placed in the sulcus of digits two through four (Figure 3). A crest pad is an easily fabricated, two-inch cotton roll (dental roll) that is placed under the interphalangeal joints of the lesser toes, on the plantar aspect. The crest pad reduces the hammertoe deformity by straightening the toes when the foot is load-bearing.5
FIGURE 3.

Lateral view of crest pad beneath second and third metatarsals.
The use of conservative treatment in older patients with varying degrees of fixed deformity has generally been disappointing. In a nonreducible hammertoe, the crest pad can cause further discomfort for the patient by accentuating the deformity; these deformities may respond to a gel-filled corn pad placed over the offending interphalangeal joint. If nonreducible hammertoes do not respond to conservative management, surgical correction should be considered.
Callus
A callus is a broad-based or diffuse hyperkeratotic lesion of relatively even thickness, usually found under the metatarsal heads at a site of friction, irritation, and pressure. Unlike corns, the margins of a callus are undefined.4 The two basic types of calluses are the diffuse-shearing (Figure 4) and the discrete-nucleated (Figure 5).
FIGURE 4.
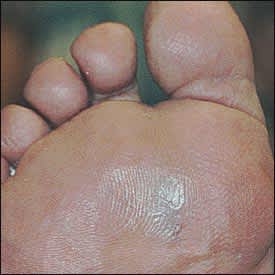
Diffuse-shearing hyperkeratotic lesion under second metatarsal head.
FIGURE 5.

Keratin plug is removed with a chisel blade.
The discrete-nucleated callus, which is often confused with the plantar wart, is often referred to as a plantar corn because this localized and painful lesion contains a central keratin plug.6 Palpation of the lesion can help differentiate the wart from the plantar corn. Plantar corns are more sensitive to direct pressure of the lesion, while a plantar wart is more sensitive on lateral compression of the lesion.7
Sharp debridement and a palliative course of treatment for both warts and calluses can define the underlying etiology of the lesion as being either mechanical or viral. Warts, unlike mechanical lesions, tend to bleed on sharp debridement. If small black or brown dots are visible after removal of the hyperkeratotic tissue, thrombosed blood vessels have become entrapped in the cylindrical projections formed by the virus.2
Pathogenesis
Abnormal mechanical stresses on the skin will result in the formation of an accumulation of several layers of the horny layer of epithelium (hyperkeratosis). Abnormal mechanical stresses can result from a variety of intrinsic factors (bony prominences or hammertoe deformities) or extrinsic factors (tight shoes, irregularities within the shoe, or high activity levels). As mechanical stresses on the skin increase, the body attempts to protect irritated skin by forming a hyperkeratotic lesion, such as a corn or a callus; however, this lesion will increase the pressure in a tight shoe, thus creating a vicious cycle: increased pressure increases the formation of corns or calluses, which further increases the pressure.8
Treatment
Hyperkeratotic lesions are secondary to increased mechanical stress and are not a disease of the skin. The principles of treatment should be to (1) provide symptomatic relief; (2) determine the mechanical etiology; (3) formulate a treatment plan that includes padding and modification of footwear; and (4) consider surgery if conservative measures fail.
SYMPTOMATIC RELIEF
A mainstay of palliative treatment is sharp debridement to reduce the amount of hyperkeratotic tissue. A chisel blade or number 15 blade may be used to pare down these lesions and remove the keratin plug, providing almost complete relief to the area (Figure 5). A pad may be used to prolong the relief provided by sharp debridement. Patients who present with diffuse hyperkeratotic lesions that are not painful may be advised to use a pumice stone to reduce the lesion after first soaking the foot in warm water. Over-the-counter products that contain salicylic acid should be avoided because they may damage surrounding normal tissues, especially in neuropathic and immunocompromised patients.4
PADDING
Therapeutic padding can alleviate the patient's symptoms by reducing the amount of mechanical irritation to the site of the corn or callus. For hard corns, foam pads or silicone toe sleeves offer the cushioning and protection needed after adequate debridement of the corn. Silicone sleeves can be especially beneficial because they cushion the foot while slowly releasing mineral oil to soften the keratotic lesion (Figure 6). After debridement of soft corns, relief can be provided by padding the web space with a foam toe spacer or a small amount of lamb's wool.4
FIGURE 6.

Silicone sleeve on fifth metatarsal.
Plantar calluses caused by weight-bearing stresses on the metatarsal heads may be relieved or eliminated by accommodative metatarsal pads. Adhesive felt (one-eighth inch to one-fourth inch) can be used to transfer weight away from the painful area and to the uninvolved areas of the foot. The size and shape of the metatarsal heads must be considered when fashioning the accommodative pad. The anterior edge of the metatarsal pad must be the full width of the metatarsal heads and narrowed proximally along the medial and lateral borders. Full width occurs at the ball of the foot. The pad becomes more narrow on each side as it approaches the heel. Small, semicircular cuts large enough to accommodate the metatarsal heads are made into the distal edge of the pad. Accommodative cuts may be made for any one metatarsal head or any combination of metatarsal heads (Figure 7). Felt padding may be applied directly on the foot or within the shoe.5
FIGURE 7.

Metatarsal pad with first and fifth head accommodations.
FOOTGEAR
Most mechanical lesions can be conservatively managed with an adequate shoe. Patients should be advised to wear low-heeled shoes with a soft upper portion and a roomy toebox.1 Patients with hammertoe deformities may need a shoe with an extra depth to accommodate hard corns that often occur on the top of the deformed toe. Patients with soft or hard corns on the fifth toe may benefit from a shoe that has extra width. Irregularities within the shoe should not be overlooked, because a poorly-positioned seam or stitching may be the mechanical irritation responsible for creating the lesion.4
SURGERY
Surgery should concentrate on correcting the abnormal mechanical stresses and should only be considered after conservative measures have failed. The goal of surgical correction of a hammertoe deformity, claw toe deformity, or mallet toe deformity is to reestablish a rectus alignment of a toe that is also free of painful lesions.9 Hard corns on the fifth toe and soft interdigital corns can be treated by resection of the prominent condyles or excision arthroplasty of the proximal phalanx of the fifth toe. Calluses under the metatarsal heads are best managed conservatively because metatarsal osteotomies have unpredictable results, and the callous may transfer to an adjacent metatarsal head.10
