Interventional radiologists have been performing image-guided spinal procedures for many years. Percutaneous vertebroplasty is a newer technique in which a medical grade cement is injected though a needle into a painful fractured vertebral body. This stabilizes the fracture, allowing most patients to discontinue or significantly decrease analgesics and resume normal activity. The impact of this procedure on the morbidity and expense associated with symptomatic osteoporotic vertebral compression fractures in the United States may be significant. Patients who are unresponsive to conservative therapy of bed rest, analgesics, and back bracing should be considered for vertebroplasty. This procedure is contraindicated in patients with active infection, untreated coagulopathy, and certain types of fracture morphology. Because many patients have multiple chronic fractures, there should be a strong correlation between the physical examination signs, symptoms, and cross-sectional imaging findings. The success rate for this procedure in treating osteoporotic fractures is 73 to 90 percent. Vertebroplasty can effectively treat aggressive hemangiomas of the vertebral body and may be palliative in patients with malignant pathologic fractures. Significant complications of the procedure are less than 1 percent.
Despite recent advances in medical therapy for osteoporosis, osteoporotic vertebral fractures remain a common problem of patients seen by family physicians. According to the Osteoporosis Foundation, 10 million people have osteoporosis, including 45 percent of white women over 50 years of age. An estimated 700,000 osteoporosis-related vertebral compression fractures occur annually, resulting in 150,000 hospitalizations.1 In 1995, the cost of treatment of vertebral fractures in the United States was $746 million.1 With an increasing life expectancy and the aging of the “baby boomer” generation, the incidence and costs of osteoporosis are expected to increase substantially.1
Osteoporotic vertebral compressions usually remain subclinical and progress gradually; however, some patients develop an acute severe pain syndrome with limited mobility and functional deterioration.
Traditional treatment of painful compression fractures has included bed rest, oral or parenteral analgesics, muscle relaxants, external back-bracing, and physical therapy.2 Calcitonin also appears to have a variable analgesic effect in osteoporotic compression fractures.3 The majority of patients respond favorably to traditional treatment; however, there are some patients who fail with conservative therapy and suffer from prolonged pain and immobility, which can persist for life.
Complications of vertebral compression fractures include the following: deep venous thrombosis; acceleration of osteoporosis; loss of height; respiratory or gastrointestinal disturbances; and emotional and social problems secondary to unremitting pain and loss of independence. Interventional procedures that shorten recovery time and eliminate the need for extended nursing and rehabilitation care should significantly decrease the high costs of treating osteoporotic vertebral fracture.4
Percutaneous vertebroplasty is a newer technique in which acrylic cement is injected through a needle into a collapsed or weakened vertebra to stabilize the fracture. This procedure is effective for treating certain types of painful vertebral compression fractures and some painful or unstable benign and malignant vertebral lesions that fail to respond to the traditional conservative therapies. Most experts believe that pain relief is achieved through mechanical support and stability provided by the bone cement. The semisolid mixture of polymethylmethacrylate (PMMA), an acrylic cement used in orthopedic procedures, has been shown to restore strength and stiffness in vertebral bodies in postmortem studies.5
The cements used for vertebroplasty have had a proven safety record in orthopedics since their first use in the 1960s.6 Nevertheless, research is still being conducted to develop better injectable bone augmentation materials and biodegradable or bioactive bone “pastes.”7,8 Ideally, these substances will strengthen the vertebral body while inducing new bone growth.
History
The first vertebroplasty was performed in 1984 by French radiologists for treatment of a painful hemangioma in the cervical spine of a young female patient.9 Since the mid-1980s in France and the mid-1990s in the United States, radiologists have been successfully treating pathologic vertebral fractures secondary to osteoporosis, painful vertebral metastasis, and multiple myeloma.10
The currently accepted indications for percutaneous vertebroplasty are listed in Table 1. The absolute and relative contraindications for percutaneous vertebroplasty are listed in Table 2.
TABLE 1 Indications for Percutaneous Vertebroplasty
| Osteoporotic vertebral compression fractures more than two weeks old in the cervical, thoracic, and lumbar spine causing moderate to severe pain and unresponsive to conservative therapy |
| Painful metastasis and multiple myelomas with or without adjuvant radiation or surgical therapy |
| Painful vertebral hemangiomas |
| Vertebral osteonecrosis |
| Reinforcement of a pathologically weak vertebral body before a surgical stabilization procedure |
TABLE 2 Contraindications for Percutaneous Vertebroplasty
| Absolute |
| Osteoporotic vertebral fracture that is completely healed or is clearly responding to conservative management |
| Presence of untreated coagulopathy |
| Presence of discitis/osteomyelitis or sepsis |
| Relative |
| Significant compromise of the spinal canal by retropulsed bone fragment or tumor |
| Fracture older than one year |
| Greater than 80 to 90 percent collapse of the vertebral body |
Pre-Vertebroplasty Work-up
The diagnosis of vertebral compression fractures is usually straightforward. Plain radiographs are obtained. Then, history and physical examination are performed to correlate the location of pain and tenderness with the level of the compression fracture and to exclude the presence of focal neurologic deficit or myelopathy.
Cross-sectional imaging, magnetic resonance imaging (MRI), or computed tomographic (CT) scanning is required to determine if there is significant spinal canal compromise, to assess the integrity of the posterior vertebral body wall, and to exclude other causes of back pain (Figure 1).
FIGURE 1.

A T1-weighted midsagittal magnetic resonance imaging scan showing a compression fracture at T12 that has normal bone marrow signal and is not acute (black arrow). A second compression at L2 has abnormal bone marrow signal indicating an acute fracture (white arrow).
Complex or multiple compression fracture patterns require careful correlation between physical examination and imaging studies before initiation of treatment.
Procedure
Vertebroplasty is most commonly performed in the angiography/interventional radiology suite. High-quality fluoroscopy is a prerequisite. Midazolam (Versed), fentanyl (Duragesic), or other medication may be administered to provide moderate sedation. Patients who are in severe pain may require general anesthesia to tolerate the prone positioning required for this procedure.
Using sterile technique and fluoroscopic guidance, an 11-gauge needle is advanced into the vertebral body via a transpedicular or parapedicular approach.
Under careful fluoroscopic visualization, PMMA cement and sterile barium or tungsten powder opacifier is slowly injected into the vertebral body, diffusing throughout the intertrabecular marrow space. The procedure is usually repeated through the contralateral pedicle unless there is adequate cross-filling of the vertebral body by the initial injection (Figure 2). The total volume of injected cement ranges from four to 12 cm.3 The cement sets in less than one hour and should stabilize the vertebra by forming a hard internal “cast.”
FIGURE 2.

A postinjection computed tomographic image shows the cement filling the fractured vertebral body.
Following the procedure, the patient is instructed to lie flat in the supine position for one hour to allow the cement to harden. Observation in the hospital should be continued for at least one to two hours, at which point most patients will be able to stand and walk with minimal or no pain.
Before being discharged, patients should be assessed for relief of back pain, focal neurologic deficit, or new chest pain. Some patients may require nonsteroidal anti-inflammatory drugs (NSAIDs) for procedure-related discomfort. Pain relief is often immediate but may take up to 72 hours (Figure 3). The radiologist should follow up with the patient by telephone or office visit at prescribed intervals to assess the response to treatment and the durability of the results.
FIGURE 3.
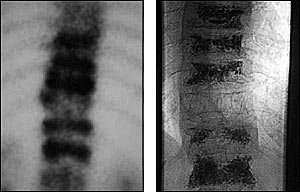
A nuclear medicine bone scan image shows multiple acute fractures in an elderly woman (left). Multiple serial vertebroplasties were necessary to achieve complete symptomatic relief in this patient (right).
Outcome Studies
Although no controlled studies comparing percutaneous vertebroplasty with conservative therapy for the treatment of osteoporotic vertebral fractures have been performed, multiple case studies and series have demonstrated positive outcomes.
One study11 showed that 90 percent of patients (29 patients with 47 fractures) with age-related or steroid-induced osteoporosis experienced pain relief and improved mobility at 24 hours post-vertebroplasty. No worsening of pain postprocedure was reported.11 Another study12 showed significant pain reduction and improvement in health profile scores of 16 patients treated at 20 vertebral levels. A third study13 described complete or partial pain relief in 97 percent of patients who were treated for painful metastasis (29 patients) and multiple myeloma (8 patients).
A series14 of 289 vertebrae in 105 patients who were treated with percutaneous vertebroplasty for a variety of lesions showed favorable outcomes in 78 percent of patients with osteoporotic lesions, 83 percent of patients with malignant lesions, and 73 percent of patients with vertebral hemangiomas. Results of a study10 on percutaneous vertebroplasty in 231 patients showed a 90 percent success rate in the treatment of osteoporotic vertebral fractures and an 80 percent success rate in painful or unstable neoplastic lesions and vertebral hemangiomas. Another study15 reported good pain relief in 73 percent of patients with at least a 50 percent reduction in analgesic dose; this study also reported moderate pain relief in 29 percent of patients (37 patients, 52 vertebrae) with painful malignant vertebral lesions.
A local tumoricidal effect within and around the cement mass has been demonstrated in a postmortem study16 of six patients who had been treated by vertebroplasty for malignant vertebral lesions.
Complications
The complication rate associated with percutaneous vertebroplasty is 1 to 3 percent for treatment of osteoporotic fractures and 7 to 10 percent for treatment of malignant neoplasms.10,17 The majority of complications are transient and minor, and they include the following: hemorrhage; rib or vertebral posterior element fracture; transient fever and worsening of pain for several hours following the procedure caused by the heat generated by cement polymerization; nerve root irritation; cement embolization to the lungs via the paravertebral venous plexus; pneumothorax for thoracic lesions;18 and infection. Permanent complications, including those requiring decompressive surgery to remove extruded cement or repair a fractured pedicle, occur at a rate of less than 1 percent.19
Future Developments
Percutaneous vertebroplasty stabilizes and strengthens the vertebral body but does not restore the height or shape of a compressed or wedged vertebra. A modification of the vertebroplasty procedure, termed kyphoplasty is being evaluated. Kyphoplasty involves the inflation of a high-pressure balloon that is introduced through an 11-gauge needle into the vertebral centrum to restore the height and shape of the vertebral body. The resultant cavity is then filled with cement.
