Malaria is a major international public health problem, responsible for considerable morbidity and mortality around the world each year. As travel to tropical locations increases, U.S. physicians are being asked more frequently to provide recommendations for malaria prevention. An organized approach to reducing the risk of acquiring this disease is necessary. Physicians must review the itineraries of their patients in detail, paying particularly close attention to travel within malaria-endemic areas and drug-resistant zones. Appropriate chemoprophylaxis must be chosen to reduce the risk of acquiring malaria. It also is important to provide advice on the use of protective measures that reduce the risk of mosquito bites. Finally, travelers should be instructed to seek medical attention immediately if symptoms of the disease develop during or after the trip.
The growing popularity of travel to tropical locales is placing an increasing number of travelers at risk for acquiring malaria. In 1998, the World Health Organization (WHO) indicated that there were more than 270 million cases of malaria worldwide, with more than 1 million deaths caused by the disease.1,2 In the United States, approximately 1,500 cases of malaria are reported annually to the Centers for Disease Control and Prevention (CDC).3
The evolving pattern of drug resistance in malaria parasites and changes in recommendations for chemoprophylaxis present a challenge to physicians who advise patients about preventing this disease. Improving adherence to use of antimosquito measures and antimalarial medications could prevent many cases of malaria. This article provides an approach to malaria prevention in travelers. It reviews key risk factors for malaria acquisition, measures to prevent mosquito bites, and drugs approved for chemoprophylaxis.
Life Cycle of Plasmodium
To better appreciate the methods of malaria prevention, it is necessary to understand the parasite's life cycle. Malaria is transmitted through the bite of an infected female Anopheles mosquito and is caused by infection with one of four species of the protozoa Plasmodium (Plasmodium falciparum, Plasmodium vivax, Plasmodium malariae, and Plasmodium ovale).4,5
When an infected mosquito takes a blood meal during its feeding period between dusk and dawn, it injects sporozoites of Plasmodium from its salivary glands into the bloodstream of the host. The sporozoites circulate to the liver and invade hepatocytes, where they divide to form tissue schizonts and then merozoites, which escape into the bloodstream. Merozoites invade erythrocytes, differentiate into trophozoites, and divide to become blood schizonts. These then mature into merozoites which, when released from red cells, can continue the cycle in the blood.
A proportion of the sporozoites of P. vivax and P. ovale develop into dormant forms within the liver, called hypnozoites, and these can activate months to years later to release more merozoites into the bloodstream, causing a symptomatic relapse. The life cycle is completed when merozoites differentiate into sexual forms called gametocytes. The female Anopheles mosquito ingests gametocytes during a blood meal, and sexual stages result in the development of sporozoites that can be transmitted to the next susceptible human host.
Approach to Malaria Prevention
The risk of malaria can be reduced by regular use of measures that limit contact with mosquitoes and by strict adherence to chemoprophylaxis.6 To help travelers adhere to these recommendations, physicians must provide complete pre-travel advice. Even a brief exposure in an endemic area puts the unprotected traveler at risk. Because no preventive regimen is completely effective, travelers also should know to seek medical attention immediately should they become febrile during or after their trip.
The approach to malaria prevention should incorporate the following principles:
- Assess the risk of malaria infection on the basis of the patient's itinerary.
- Discuss the available methods of reducing contact with Anopheles mosquitoes.
- Identify the most appropriate antimalarial agents for chemoprophylaxis.
- Alert the traveler to seek early diagnosis and treatment if fever develops during or after travel.
These principles provide a framework for the physician to follow when counseling patients about malaria prevention during pre-travel office visits. Figure 1 illustrates an algorithmic approach to the prevention of malaria in travelers.
FIGURE 1. Overall Approach to Malaria Prevention
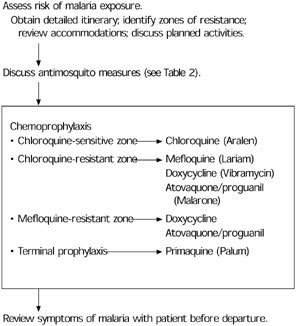
Algorithm for preventing malaria in patients traveling outside the United States.
Assessing the Risk of Malaria
Assessing malarial risk requires a detailed knowledge of a patient's travel itinerary and accommodations. The risk that a traveler will become infected depends on the overall rate of malaria transmission in the geographic area to be visited and on the extent of the patient's contact with infected mosquitoes.7 Transmission rates vary greatly from region to region, even within the same country. In countries where the overall risk is relatively low, there may be foci of intense transmission.
The assessment of risk of malaria infection depends on several other considerations. Because malaria transmission often follows stringent seasonal patterns linked to rainfall, the timing of the trip may influence the risk.8 The elevation of the destination also is important because malaria transmission is rare above 2,000 m (6,561 feet).9 Finally, because the Anopheles mosquito feeds from dusk to dawn, the risk of transmission is influenced by a traveler's nighttime activities and accommodations.
Regularly updated maps identifying malaria risk areas and times are available from several sources (Table 1)10 and can be valuable tools in counseling patients.11 Details about risk within countries may be obtained from Web sites operated by the CDC (www.cdc.gov/travel) and the WHO (www.who.int/ith).
TABLE 1 Malaria Prevention Resources
| CDC contacts |
| Voice information system: 888-232-3228 |
| Fax information system: 888-232-3299 |
| Malaria Hotline: 770-488-7788 |
| Books |
| CDC. Health Information for International Travel 2001–2002. Atlanta: U.S. Department of Health and Human Services, Public Health Service, 2001 |
| Textbook of Travel Medicine and Health, by Herbert L. DuPont and Robert Steffen. Hamilton, Ontario: B.C. Decker, Inc., 1997 |
| The Travel and Tropical Medicine Manual, by Elaine C. Jong and Russell McMullen, eds. 2d ed. Philadelphia: W.B. Saunders, 1995 |
| Web sites |
| CDC Travelers' Health Information: www.cdc.gov/travel |
| World Health Organization International Travel and Health: www.who.int/ith |
| International Society of Travel Medicine: www.istm.org |
| American Society of Tropical Medicine and Hygiene: www.astmh.org |
| Pan American Health Organization: www.paho.org |
| Malaria Foundation International: www.malaria.org |
CDC = Centers for Disease Control and Prevention.
Adapted from Health information for international travel 2001–2002. Atlanta: U.S. Department of Health and Human Services, Public Health Service, 2001.
Protection Against Mosquitoes
The most effective protection against malaria is to avoid exposure to the Anopheles mosquito that carries the disease.6,8 All travelers to malaria-endemic areas should be instructed on how best to avoid bites from these mosquitoes. A significant reduction in the risk of acquiring the disease can be achieved by simply limiting evening exposure to mosquitoes.
Travelers in endemic areas can substantially reduce the probability of infection with certain behavior adaptations. Wearing clothes that minimize the amount of exposed skin is helpful. The use of insect repellent on exposed skin should be encouraged. Repellents containing N, N-diethyl-3-methylbenzamide (DEET) in concentrations of approximately 30 percent are effective and safe.12,13 DEET has been used safely by millions of people worldwide but has been noted to cause urticaria, irritation of the eyes, or headaches on rare occasions.12 Spraying with an ordinary household insecticide can knock down mosquitoes already in small, enclosed spaces such as a hotel room or tent. Finally, because mosquitoes are not strong fliers, use of a room fan can keep them out of the air.
Persons who will not be staying in rooms that are well screened or air-conditioned should consider sleeping under a mosquito bed net. The use of bed nets has been reported to reduce the mosquito attack rate by 97 percent.14 [evidence level A, randomized controlled trial (RCT)] Bed nets and sleeping bags impregnated with an insecticide such as permethrin should be used because they are effective barriers to vectors even if torn.6,15,16 [Reference 16—evidence level B, cross-sectional study] Table 2 provides a summary of protective measures against mosquitoes.
TABLE 2 Personal Protective Measures Against Mosquito Bites
| Minimize outdoor activities between dusk and dawn when Anopheles mosquitoes commonly bite. |
| Wear long-sleeved shirts and long trousers. |
| Apply insect repellent containing approximately 30 percent N, N-diethyl-3-methylbenzamide (DEET) to exposed skin at dusk. Repeated application may be required every three to four hours. |
| Stay in a building with air-conditioning or with screens over doors and windows. If no screens are available, windows and doors should be closed at sunset. |
| Apply aerosolized insecticides in living or sleeping areas at dusk. |
| Use a strong fan to inhibit the flight of mosquitoes. |
| Use a mosquito bed net, preferably one that is impregnated with permethrin, if accommodation allows entry of mosquitoes. Bed nets can be soaked in this insecticide solution and hung out to dry. They should be retreated every six months to maintain effectiveness. |
Chemoprophylaxis
A number of medications have been shown to have efficacy in preventing malaria infection. As with all treatments, the use of an antimalarial regimen should involve balancing the potential adverse effects against the risk of acquiring malaria.8 Contraindications to the use of specific antimalarial agents for specific patients should be identified. Table 3 summarizes the current recommended chemoprophylactic agents.10
CHLOROQUINE
Because of the emergence of drug-resistant P. falciparum strains, chloroquine (Aralen) is no longer the recommended chemoprophylaxis medication in most parts of the world. Chloroquine is still recommended for prophylaxis in travelers to Central America west of the Panama Canal, Hispaniola (Haiti and the Dominican Republic), Argentina, parts of China, and parts of the Middle East (primarily Syria, Jordan, and Iraq).10 [evidence level C, consensus/expert guidelines]
TABLE 3 Drugs for Prophylaxis of Malaria
| Drug | Usage | Adult dosage | Cost* | Comments |
|---|---|---|---|---|
| Chloroquine (Aralen) | In areas with chloroquine-sensitive Plasmodium falciparum; safe option in pregnancy | 500 mg orally, once a week; begin therapy two weeks before exposure and continue for four weeks after. | $ 5.26 | — |
| Mefloquine (Lariam) | In areas with chloroquine-resistant P. falciparum; safe option in pregnancy | 250 mg orally, once a week; begin therapy two weeks before exposure and continue for four weeks after. | $10.75 | Not recommended in patients with seizure disorders, cardiac conduction abnormalities, or psychosis |
| Doxycycline (Vibramycin) | Alternative to mefloquine in areas with chloroquine- resistant P. falciparum;contraindicated in pregnancy | 100 mg orally, once a day; begin therapy two days before exposure and continue for four weeks after. | $ 4.34 | Contraindicated in lactating women and children younger than eight years; should be taken with food |
| Atovaquone/ proguanil (Malarone) | Alternative to mefloquine and adoxycycline in areas with chloroquine-resistant P. falciparum; contraindicated in pregnancy | 1 adult tablet (250 mg atovaquone/100 mg proguanil) orally, once a day; begin therapy one to two days before exposure and continue for one week after. | $ 4.70 | Contraindicated in severe renal failure (creatinine clearance less than 30 mL per minute); should be taken with food |
| Primaquine (Palum) | As terminal prophylaxis in those with prolonged exposure to Plasmodium vivax or Plasmodium ovale, or both, or exposure in areas of intense P. vivax transmission; contraindicated in pregnancy | 26.3 mg orally, once a day, for 14 days after departure from endemic area | $ 0.90 | Contraindicated in patients with G6PD deficiency; for chemoprophylaxis (not yet FDA-approved for this purpose), take 2 tablets daily one day before exposure and continue for seven days after departure from an endemic area |
G6PD = glucose-6-phosphate dehydrogenase; FDA = U.S. Food and Drug Administration.
*—Estimated cost to the pharmacist per tablet based on average wholesale prices in Red book. Montvale, N.J.: Medical Economics Data, 2001. Cost to the patient will be higher, depending on prescription filling fee.
Adapted from Centers for Disease Control and Prevention. Health information for international travel 2001–2002. Atlanta: U.S. Department of Health and Human Services, Public Health Service, 2001.
The antimalarial dosage for a traveler to these areas is one 500-mg tablet (300 mg base) per week beginning two weeks before departure, with one tablet per week during exposure, and one tablet per week for four weeks after the trip. The most common side effect is dyspepsia, but chloroquine also can cause pruritus (especially in dark-skinned persons), exacerbations of psoriasis, agranulocytosis, photosensitivity and, rarely, neuropsychiatric disturbances such as vertigo or insomnia.17,18 The drug is a safe option during pregnancy.
MEFLOQUINE
Mefloquine (Lariam) is the drug of choice for most travelers to chloroquine-resistant regions.9 The traveler takes one 250-mg tablet once per week for two weeks before departure, one tablet per week during travel, and one tablet per week for four weeks after returning home.
In the past decade, many anecdotal reports of neuropsychologic adverse effects have raised major concerns about this drug. However, adverse effects are similar in frequency and severity to those reported with weekly chloroquine use.19 The most commonly reported side effects include nausea, dizziness, headaches, and vivid dreams. Mefloquine should be used with caution in patients with a history of psychosis, seizure disorder, or cardiac conduction defects. It is the most efficacious and safe option for the prevention of malaria in pregnant women traveling to areas with chloroquine-resistant P. falciparum.10
DOXYCYCLINE
Doxycycline (Vibramycin), a tetracycline, continues to be the preferred agent for persons unable to tolerate mefloquine and for those traveling to areas where mefloquine resistance is present.1 The drug is taken in a dosage of 100 mg daily during exposure and continued for four weeks after the traveler returns home. No loading dose is required. Doxycycline has been shown to have prophylactic efficacy comparable to mefloquine, but the need for daily dosing may reduce adherence and, therefore, effectiveness.20 [evidence level A, RCT]
Side effects of doxycycline include gastrointestinal upset, esophagitis, and vaginal candidiasis. Because the drug can be photosensitizing, its use requires adequate sunscreen protection. Doxycycline is contraindicated in pregnant or lactating women and in children younger than eight years.8 Long-term administration of tetracyclines generally has been well tolerated.6
ATOVAQUONE/PROGUANIL
The U.S. Food and Drug Administration recently approved a fixed-combination tablet of atovaquone and proguanil (Malarone) for the chemoprophylaxis of malaria. Travelers need only take the medication during periods of exposure and for one week after departure from the malarial region.21 This regimen has an advantage over that of mefloquine and doxycycline, which have to be taken for four weeks following exposure.
Atovaquone/proguanil has been found to be useful against strains of malaria that are resistant to other agents.22,23 [Reference 22—evidence level B, uncontrolled clinical trial] The adult dosing regimen for prophylaxis consists of one tablet (250 mg atovaquone/100 mg proguanil) per day starting two days before travel, one tablet per day during travel, and one tablet per day for seven days after leaving an endemic area.
The most common adverse effects are abdominal pain, nausea, and headaches.21 Because of insufficient data on its safety in pregnancy, it should not be taken by pregnant or lactating women. Atovaquone/proguanil also is contraindicated in persons with severe renal impairment. This drug combination generally is well tolerated and efficacious in the prevention of P. falciparum infection. More data are needed to confirm its efficacy against other malaria species.
PRIMAQUINE
Primaquine (Palum) has activity against the blood and liver stages of malaria parasites.1 In patients who have been infected with P. vivax or P. ovale, relapses can occur long after chemoprophylaxis is discontinued because the standard drugs fail to eliminate the liver hypnozoites. To prevent relapses, a course of primaquine may be given as terminal prophylaxis at the conclusion of the standard post-travel chemoprophylaxis regimen. One 26.3-mg tablet is administered per day for 14 days after the trip. Terminal prophylaxis generally is indicated only for use in persons who have a prolonged exposure in malaria-endemic areas or who have visited areas of intense P. vivax transmission.15
Primaquine causes acute intravascular hemolysis in those with an inborn deficiency of glucose-6-phosphate dehydrogenase (G6PD). The drug should not be prescribed without confirming a normal G6PD level. Primaquine should not be used during pregnancy.
Recognition of Illness
Travelers should be informed that although antimalarial agents can markedly decrease the risk for developing symptomatic malaria, none of them can guarantee complete protection.9 Travelers should be told to seek medical attention immediately if fever develops during or after a visit to an endemic area. They should be warned that malaria is possible as early as one week after first exposure and as late as several months or even years (for P. vivax, P. malariae, and P. ovale) after returning from a trip. Symptoms of infection with P. falciparum almost always begin within two months of departure from an endemic area, but only 50 percent of persons infected with vivax malaria present in the first two months after they return home.9
Finally, travelers should be informed of the main symptoms of malaria. Fever, malaise, headaches, myalgias, arthralgias, chills, and sweats occur in more than 80 percent of patients with malaria.4 The “typical” cyclic fevers often do not occur in travelers returning to this country. Other symptoms include anorexia, nausea, vomiting, abdominal pain, and diarrhea.
