Pain in labor is a nearly universal experience for childbearing women. A recent evidence-based symposium on the nature and management of labor pain brought together family physicians, obstetricians, midwives, obstetric anesthesiologists, and childbirth educators to discuss a series of commissioned systematic reviews. Although management of labor pain plays a relatively minor role in a woman's satisfaction with childbirth compared with the quality of the relationship with her maternity caregiver and the degree of participation she has in decision making, it is an important topic for women and their caregivers. Nonpharmacologic methods of pain relief such as labor support, intradermal water blocks, and warm water baths are effective techniques for management of labor pain. An increased availability of these methods can provide effective alternatives for women in labor.
In May 2001, family physicians, obstetrician–gynecologists, anesthesiologists, nurse-midwives, and childbirth educators met at the Nature and Management of Labor Pain symposium sponsored by the Maternity Center Association and New York Academy of Medicine. Participants discussed presentations on the nature of labor pain, the history of anesthesia for childbirth, maternal satisfaction with childbirth, and the role of maternal choice. Commissioned systematic reviews focused on methods of labor pain management, including nonpharmacologic techniques, parenteral opiates, epidural analgesia, paracervical block, and nitrous oxide. Part I of this two-part article focuses on the nature of labor pain, maternal satisfaction with childbirth, and nonpharmacologic methods of pain relief.
Nature of Labor Pain
Although most women report that labor is painful, most physicians have surprisingly little understanding of the nature of labor pain. Pain is a subjective experience involving a complex interaction of physiologic, psychosocial, cultural, and environmental influences. A recent review by Lowe,1 which was based primarily on descriptive studies, focused on methods for measuring pain experience and physiologic and environmental factors that influence labor pain.
During the first stage of labor, women usually perceive the visceral pain of diffuse abdominal cramping and uterine contractions. In the second stage of labor, there is a sharper and more continuous somatic pain in the perineum. Pressure or nerve entrapment caused by the fetus's head can cause severe back or leg pain. Nulliparous women generally experience more sensory pain during early labor,2,3 while multiparous women may experience more intense pain during the late first stage and the second stage of labor, as a result of rapid fetal descent.2,4
Cultural values and learned behaviors influence perception and response to acute pain. Women's expectations about labor pain often are confirmed by their experience of childbirth.5,6 Anxiety and fear of pain correlate with a higher reported experience of pain.5–8 A woman's confidence in her ability to cope with labor is the best predictor of pain during the first stage of labor, accounting for nearly one third of the reported variance in pain.7
Women rate labor pain as more intense than their caregivers do.9 Cultural gaps between the patient and caregiver can exacerbate this difference. The birth environment affects a woman's experience of pain and her ability to cope with pain during labor. Adequately powered, prospective studies that examine the relationship between pain, birth environments, and various styles of care are needed.
Childbirth and Maternal Satisfaction
Many clinicians assume that a major determinant of maternal satisfaction with childbirth is effective pain relief during labor. There are both affective and cognitive components to maternal satisfaction.10 A woman's sense of satisfaction with her childbearing experience changes over time; when measuring maternal satisfaction, the amount of time that has elapsed since the birth may be a key methodologic factor.11
A systematic review of the literature by Hodnett11 on the relationship between the use of labor analgesia and maternal satisfaction concluded that pain relief does not play a major role in overall maternal satisfaction with the childbirth experience. Three randomized controlled trials (RCTs) included in the review did not demonstrate improved satisfaction with increased pain relief. Factors associated with increased maternal satisfaction were the quality of the relationship with the caregiver and the amount of participation in decision making during labor and delivery. The review also found that women preferred a home-like birth environment, and caregivers with whom they are acquainted personally.11
Nonpharmacologic Pain Relief in Labor
Nonpharmacologic methods of pain relief are used by virtually all women in labor. A systematic review by Simkin and O'Hara of nonpharmacologic pain relief12 examined five methods: continuous labor support, warm water baths, intradermal water injections, maternal movement and positioning, and touch and massage. Pain-relief methods without prospective studies (e.g., acupuncture) and self-help techniques such as relaxation, breathing, and visualization were not examined.
CONTINUOUS LABOR SUPPORT
Continuous labor support provided by a doula, a lay woman trained in labor support, consistently has decreased the use of obstetric interventions. A Cochrane meta-analysis (Table 1) found a decrease in operative vaginal deliveries, cesarean deliveries, and requests for pain medication when continuous labor support was given.13 [Evidence level A, meta-analysis] Fewer women had unsatisfactory birth experiences.13
TABLE 1 Evidence for Continuous Support During Labor
| Outcome | Relative risk | 95% confidence interval | NNT* | ARR (%)† |
|---|---|---|---|---|
| Use of any analgesia (all types of support providers) | 0.87 | 0.79 to 0.96 | 16 | 6 |
| Use of any analgesia (doulas or other nonhospital staff) | 0.72 | 0.49 to 1.05 | N/A | N/A |
| Operative vaginal delivery (all types of support providers) | 0.89 | 0.83 to 0.96 | 50 | 2 |
| Operative vaginal delivery (doulas or other nonhospital staff) | 0.59 | 0.42 to 0.81 | 32 | 3 |
| Cesarean delivery (all types of support providers) | 0.90 | 0.82 to 0.99 | 100 | 1 |
| Cesarean delivery (doulas or other nonhospital staff) | 0.74 | 0.61 to 0.90 | 22 | 4 |
| Birth not satisfactory to mother (all types of support providers) | 0.73 | 0.65 to 0.83 | 50 | 2 |
| Birth not satisfactory to mother (doulas or other nonhospital staff) | 0.67 | 0.58 to 0.78 | 7 | 14 |
NNT = number needed to treat; ARR = absolute risk reduction; N/A = not applicable.
*—NNT is the number of women who will need to receive the intervention to prevent a single case of the outcome.
†—ARR is the absolute risk reduction in the intervention group compared with the control group.
Information from reference 13.
Intermittent labor support does not convey the same benefits as continuous support.14 A recent large RCT demonstrated that providing continuous labor support with nurses instead of doulas had no effect on cesarean delivery rates or other birth outcomes.15 Low-income women who otherwise would labor with minimal or no social support receive the greatest benefit from a doula.12 The review notes the lack of studies of the model of doula care most commonly used in North America, in which women meet their doulas in the prenatal period.12
WARM WATER BATHS
Warm water baths increasingly are available in hospitals and birth centers. Two prospective cohort studies and seven RCTs were included in the systematic review.12 A small RCT16 that measured pain before, during, and after bathing found that pain was relieved during the bath and returned afterward. A larger RCT17 that measured pain at 24 to 48 hours and eight months postpartum found no difference in perception of pain.
Warm water baths had no effect on the use of epidural analgesia in the three largest studies,17–19 which may be because of the short duration of pain relief. None of the RCTs showed increased maternal or neonatal infectious morbidity. One RCT20 found that labor was longer when a bath was used in early labor (less than 5-cm dilation) than when it was used in late labor.
A recent, nationwide survey21 found that 6 percent of women used warm water baths during labor, and that 49 percent found them very helpful with pain relief. Warm water baths during labor seem to be safe and possibly effective for limited periods. It has been recommended that physicians wait for active labor to begin before initiating baths, maintain the water at or below body temperature, and limit bath time to one to two hours.12
STERILE-WATER INJECTIONS
Intradermal injections of sterile water in the sacral area may be used to decrease back pain in labor (Figure 1). Sterile-water injection causes a burning sensation that is much more painful than saline injection and is thought to relieve labor pain by counterirritation. Four RCTs included in one review12 found a significant reduction in back pain for 45 to 90 minutes based on a visual analog scale. Three of the trials found that women who received injections of sterile water were more interested in receiving the injections in a subsequent labor than women who received saline injections. None of the trials showed a decrease in requests for pain medicines, perhaps because of the limited time of effectiveness or a lack of effectiveness for abdominal labor pain.
FIGURE 1.
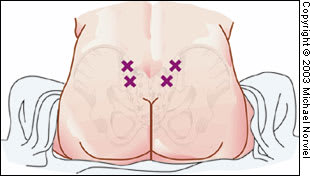
Intradermal injections of 0.1 mL of sterile water in the treatment of women with back pain during labor. Sterile water is injected into four locations on the lower back, two over each posterior superior iliac spine (PSIS) and two 3 cm below and 1 cm medial to the PSIS. The injections should raise a bleb below the skin. Simultaneous injections administered by two clinicians will decrease the pain of the injections.
POSITIONS, TOUCH, AND MASSAGE
When women are not restricted by caregivers or institutional policies, they commonly assume a variety of positions during labor. Fourteen RCTs included in one review12 failed to show consistent findings regarding position and labor pain. Only one of seven RCTs in which women were randomized to various positions showed a decrease in the use of analgesia.12
Two trials of touch and massage during labor met the criteria for the systematic review. The studies were small and have methodologic problems that prevent reaching a conclusion on the effect of touch and massage on labor pain.
