to the editor: A 67-year-old night watchman was referred to our clinic by an ophthalmologist because of a one-month history of recurrent vertical diplopia. The diplopia usually occurred after work when he was exhausted or after he had consumed sake. The diplopia always resolved spontaneously after sleeping, but this time it persisted for several weeks, and he finally consulted an ophthalmologist.
On examination, his right eye was higher than the left, which produced the vertical diplopia, but there was no facial swelling (Figure 1). Three-dimensional computed tomography showed a complete bone defect in the orbital floor and a mucocele (red) displacing the eyeball (blue) superiorly (Figure 2), which resulted in the symptom of vertical diplopia. Despite the defect in his orbital floor, the periosteum was intact. The mucocele was drained by aspiration (needle aspiration) through the gingivobuccal sulcus. After removing 20 mL of mucus, the right eye returned to the same level as the left eye, and the diplopia resolved completely. The aspirated mucus had no bacterial infection and the cytologic study showed no malignancy.
A Caldwell-Luc surgical technique had been performed on this patient for right maxillary sinusitis 30 years earlier, but the nasoantral window for drainage had gradually narrowed. The mucosal lining of the sinus continued to produce mucus, and it became swollen during and after inflammation (consuming alcohol) and pushed the eyeball superiorly. The diagnosis was postoperative maxillary sinus mucocele.
Figure 1

Patient with vertical diplopia (right eye higher than the left).
Figure 2
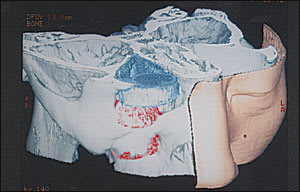
Three-dimensional computed tomography showing a complete bone defect in the orbital floor and a mucocele (red) displacing the eyeball (blue) superiorly.
Postoperative maxillary sinus mucocele is rare in the United states and Europe1–3 ; however, it is common in Japan.4.5 It typically occurs 10 to 15 years after the initial Caldwell-Luc operation and is accompanied by a swollen and painful cheek.5 Interestingly, this patient had never complained of a swollen and painful cheek. Even without those symptoms, recurrent diplopia would occur. The history of sinus surgeries is important to detect in such cases.
Currently, we are planning to reoperate on the right maxillary sinus to provide permanent drainage by an endoscopic sinus surgery. However, the patient’s liver function does not permit use of general anesthesia, because of chronic hepatitis.
