At least three models have been used to project the future physician workforce, and each produces different results. No physician workforce predictions can be relied on until there is more consideration of and agreement on desired health outcomes and what physicians must do to achieve them.
In the current debate on whether to expand the U.S. primary care physician workforce, three different models have been used: the supply-demand (extrapolation) model, the trend (extrapolation) model, and the need (expert) model. The results from each are dramatically different, leading to much controversy.1 Researchers at one end of the spectrum forecast sufficiency and thus would focus on improving the quality and distribution of the workforce at its current level, whereas those at the other end forecast shortages by 2020 and advocate expansion. The accompanying figure1–3 illustrates how forecasts differ with the three models. Annual growth rates are 3.2, 2.1, and 0.8 percent as projected with the supply-demand, trend, and need models, respectively.
The results of projections differ because the models are based on different assumptions. The supply-demand model assumes medical residency positions can increase in response to an expected rate of economic growth. The trend model assumes that existing trends, policies, and training positions will be maintained, thus expecting and accounting for no future changes in market factors. The need model assumes the number of physicians should match the calculated number required to provide medical services to the future population.4 The models also differ in limitations, implications for population health outcomes, and resource costs.
Figure. U.S. Family Physician Workforce Forecasts, 2005 to 2020
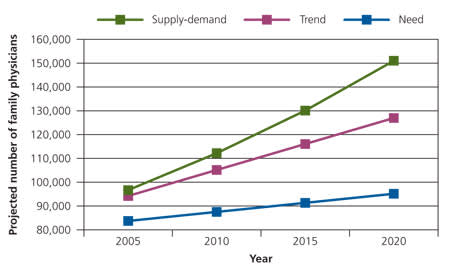
Forecasts of the U.S. family physician workforce, 2005 to 2020, using three models.
Information from references 1 through 3.
The United States ranks near the bottom of developed countries in terms of the health of its population. Instead of continuing to debate workforce expansion, physician workforce planning should consider how we can improve health care for everyone in the United States and what workforce would be needed to do so. Only when we agree on desired health outcomes (e.g., improved health status; reduced infant mortality; lower mortality from cancer, heart disease, and stroke) and the composition of a workforce that could achieve them can realistic projections be determined.
