Otitis externa can take an acute or a chronic form, with the acute form affecting four in 1,000 persons annually and the chronic form affecting 3 to 5 percent of the population. Acute disease commonly results from bacterial (90 percent of cases) or fungal (10 percent of cases) overgrowth in an ear canal subjected to excess moisture or to local trauma. Chronic disease often is part of a more generalized dermatologic or allergic problem. Symptoms of early acute and most chronic disease include pruritus and local discomfort. If left untreated, acute disease can be followed by canal edema, discharge, and pain, and eventually by extra-canal manifestations. Topical application of an acidifying solution is usually adequate in treating early disease. An antimicrobial-containing ototopical is the preferred treatment for later-stage acute disease, and oral antibiotic therapy is reserved for advanced disease or those who are immunocompromised. Preventive measures reduce recurrences and typically involve minimizing ear canal moisture, trauma, or exposure to materials that incite local irritation or contact dermatitis.
Otitis externa (OE) can take acute or chronic forms. The acute form is primarily of bacterial origin and annually affects four in 1,000 persons in the United States. The chronic form is commonly of a fungal or allergic origin or is the manifestation of dermatitides. It affects 3 to 5 percent of the population.1–4 Acute OE is unilateral in 90 percent of patients; it peaks in persons seven to 12 years of age, declines after 50 years of age, and often is associated with high humidity, warmer temperatures, swimming, local trauma, and hearing aid or hearing protector use.5
Manifestations include pruritus, pain, and erythema, but as the disease progresses, other problems such as edema, otorrhea, and conductive hearing loss may develop. Disease can range from mild inflammation, which occurs in approximately 50 percent of cases, to life-threatening temporal bone infections in less than 0.5 percent.2,4,6 Chronic OE is characterized by pruritus, mild discomfort, and an erythematous external canal that may or may not be lichenified. For both types, treatment includes topical therapy and amelioration of inciting factors. Although this is adequate therapy in most patients, at least 25 percent will be given an oral antibiotic.4,7,8
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References | Comments |
|---|---|---|---|
| Clear any obstructing debris or excess cerumen from the canal and check the integrity of the tympanic membrane and manifestations of the infection that have spread beyond the ear canal. | C | 3–5,9,19 | Use suction or curette/spoon device rather than irrigation until intact tympanic membrane is visualized. |
| Relieve pain and discomfort with analgesics. | A | 4,19,22,24 | Acetaminophen or nonsteroidal anti-inflammatory drugs if mild to moderate; consider opioids if severe. |
| Use acidifying drops if there is mild inflammation, and consider antimicrobial drops if the disease is more advanced. | C | 3,12,17,23 | Select antibacterial versus antifungal agent based on clinical appearance. |
| Add oral antibiotic if there is severe disease in an immunocompetent patient or if there is moderate or severe disease in those who are immunocompromised, who have diabetes or advanced age, and in patients with concomitant otitis media. | C | 3,4,9,22 | Consider possibility of malignant external otitis if there is severe pain, a temperature higher than 102.2°F (39°C), necrosis of canal skin, auricular chondritis, cervical adenitis, parotitis, facial paralysis, vertigo, or profound hearing loss. |
| Counsel the patient about preventive measures. | C | 5,9,30–32 | Dry ear canals after swimming or use prophylactic acidifying drops; avoid using cotton swabs or locally sensitizing agents. |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, see page 1463 orhttps://www.aafp.org/afpsort.xml.
Pathophysiology
The ear canal is a skin-lined, 2.5-cm cul-de-sac. The lateral 33 percent of the canal has a cartilaginous infrastructure covered by a layer of sebaceous and apocrine glands and hair. The medial canal has an osseous support devoid of adnexal structures. The glands produce a thin layer of cerumen that provides protection via a modestly antimicrobial lysozyme. The cerumen also has a pH level of 6.9, which discourages microbial growth.2,5,9,10 Insufficient cerumen predisposes to infection, whereas thickened cerumen, which can be caused by genetics, metabolism, or age, fosters retention of water and debris.5,9,10 Ear canals self-clean via a lateral epithelial migration towards the external os, a process that slows with age.
Before World War II, fungi were thought to be the primary cause of acute OE, but research by the U.S. military in the South Pacific confirmed a predominantly bacterial process as the cause.5,11 Approximately 50 percent of bacterial cases involve Pseudomonas aeruginosa, followed in incidence by Staphylococcus aureus and then various aerobic and anaerobic bacteria.3,6,12,13 The incidence of fungal infection is only 10 percent. Less than 5 percent of acute disease cases can be attributed to furunculosis (usually staphylococcal), herpes zoster oticus, or nonspecific conditions (e.g., bullous myringitis).2,5,9
Signs or symptoms lasting three months or longer indicate chronic OE. Although it can result from inadequately treated acute OE, it is usually of nonbacterial origin.1,4,14,15 A common cause of chronic OE is allergic contact dermatitis from such things as metal earrings, chemicals in cosmetics or shampoos, or the plastic in hearing aids or protection devices. Generalized skin conditions such as atopic dermatitis (i.e., eczema) or psoriasis can be difficult to treat in the narrow ear canal. Food sensitivity is a potential origin of chronic OE associated with atopic dermatitis in up to 48 percent of patients.4,14
A variant of chronic OE is a type IV cell-mediated hypersensitivity reaction to components of an ototopical used to treat acute OE.1,9,15 Dermatophytid eruptions also can manifest in the canal and are reactions to hematogenously spread fungal by-products from a primary focus (e.g., nails, scalp, or vagina).1 A subtype of chronic OE is reported in 6 to 40 percent of patients following insertion of a pressure equalization tube that leads to middle ear drainage, purulent or not, causing canal maceration.13,16–18
Evaluation
The onset of acute OE generally is over a few days to a week. Initially it is characterized by a scant, odorless secretion as well as mild discomfort and pruritus associated with modest erythema. If disease progresses to a moderate stage, the erythema increases and is joined by edema (particularly in the thicker lateral canal), seropurulent secretions, and pain exacerbated by tragal pressure or movement of the auricle (Figure 1). In the severe stage, pain is intense, the lumen of the canal obstructed, and extra-canal signs such as auricular cellulitis, parotitis, or adenopathy are likely.2,4–6,9
Figure 1.

Acute otitis externa with the canal somewhat narrowed from edema and obstructed by desquamating epithelium, soft cerumen, and purulent discharge; this must be removed to visualize the tympanic membrane and to allow ototopical therapy to penetrate to all the superficially infected areas of the canal skin.
Evaluation includes taking a history of the onset and nature of symptoms; and of prior issues with skin disorders or local trauma, particularly via cotton swab or bobby pin. Patients with diabetes, those who are immunocompromised, and those with local circulatory insufficiency (e.g., from irradiation) are prone to rapid escalation from mild to severe manifestations.3 Regardless of the ototopical selected, penetration to the epithelium is mandatory; any obstruction should be cleared. Examination includes the ear canal, tympanic membrane, the auricle, and cervical nodes, as well as a cutaneous survey for other dermatologic manifestations. Cerumen or debris that blocks the canal is cleared to verify tympanic integrity. Concomitant and often erroneous diagnoses of acute OE and otitis media are common because the tympanic membrane in acute OE often is erythemic.8,9,19
Pneumatic otoscopy helps rule out middle ear disease. Debris usually can be cleared with a small Frazier suction tip (5 or 7 Fr) or an ear curette or spoon. Lavage is avoided until tympanic integrity is documented. Cerumen in acute OE tends to be hydrated by the otorrhea, making it easier to remove. If the cerumen is thick or otherwise adherent, or if the patient is intolerant, a liquid ototopical used overnight can aid in loosening canal debris.
Treatment
Topical therapy for canal disease was described more than 3,000 years ago; astringents and alcohols were common.5,11,20 Two percent acetic acid (Vosol), sometimes diluted in half by 90% to 95% alcohol, is effective for prophylaxis against acute OE and, with or without the addition of a steroid, for the treatment of mild disease. The caveat is that these solutions can cause stinging and irritation if applied to highly inflamed skin.2–4,8–10,19–22
More advanced disease warrants the use of an ototopical that includes an antimicrobial agent (Table 1). Regardless of the ototopical selected, penetration to the epithelium is mandatory; any obstruction should be cleared. Warming the ototopical to body temperature (e.g., by placing it in a shirt pocket or a warm room) before application helps the patient avoid the dizziness from caloric stimulation that cold liquid can incite. Instructing the patient to lie on his or her side with the affected ear up for a few minutes after the administration of ear drops aids migration to the medial canal. Having the patient or someone else pump the tragus a few times improves this process. There is wide variability in the self-administered dosing of ear drops, and relying on another person to place the drops or to perform the pump maneuver better standardizes the process.8,9,21,23
TABLE 1 Common Ototopicals for the Treatment of Otitis Externa
| Agent | Comments |
|---|---|
| 2.0% acetic acid (Vosol), with or without steroid | Inexpensive; effective for mild acute OE of bacterial or fungal origin in immunocompetent patients; typically combined with steroid if used for acute OE, but not for prophylaxis; best applied every four to six hours; can sting and locally irritate |
| 2.75% boric acid or 90% to 95% isopropyl alcohol | Inexpensive; effective for mild acute OE of bacterial or fungal origin in immunocompetent patients, but mainly applied as prophylaxis after swimming; alcohol commonly mixed 50/50 with 2% acetic acid because the alcohol evaporates quickly and affords a drier ear canal; can sting and locally irritate |
| Aminoglycoside | Moderately expensive; usually ophthalmic preparation (e.g., gentamicin, tobramycin [Tobrex]) but effective for bacterial acute OE; best applied every six hours; minimally irritating; ototoxic potential |
| Neomycin, polymyxin B, hydrocortisone | Relatively inexpensive; effective for acute OE of bacterial origin; best applied every six hours; neomycin sensitizing in 5 to 18 percent of patients; ototoxic potential |
| Fluoroquinolone, with or without steroid | Moderately expensive to expensive; effective for bacterial acute OE; best applied twice daily; minimally irritating and infrequently sensitizing; only agent approved if tympanic membrane is perforated |
| Steroid | Inexpensive to moderately expensive; addresses underlying dermatitis (e.g., atopic dermatitis, psoriasis) if it is the cause of chronic OE; solution easier to apply than cream; application frequency depends on agent selected; cutaneous atrophy with prolonged use |
| Tolnaftate (Tinactin) or clotrimazole (Lotrimin) | Relatively inexpensive; meant for general cutaneous use but effective for acute or chronic OE of fungal origin (whether primary or from suprainfection after antibacterial ototopical); solution easier to apply than cream; best applied every six hours; minimally irritating |
| Various agents: chloroxylenol (Tri-Otic), an antiseptic; pramoxine (Prax), an anesthetic; benzocaine (Americaine), an anesthetic | Few data published about effectiveness; all can incite contact dermatitis; topical anesthetics can mask symptoms of advancing infection |
OE = otitis externa.
A cotton ball temporarily placed in the external os before the patient reassumes an erect position will absorb excess liquid. If the canal is narrowed at least 50 percent by edema, placement of a wick (which can be anything from gauze to a preformed cellulose sponge) ensures ototopical access to the medial canal. When indicated, a return visit in two to three days for removal of the wick is necessary. Ototopical therapy usually should continue for five to 10 days depending on disease severity, or for three days after the last symptoms.
For other than mild acute OE, analgesics are appropriate treatment and can range from nonsteroidal anti-inflammatory drugs to mild narcotics.4,8,9,19,24 The ototopical should include an active antimicrobial agent, not just an inhibitor such as acetic acid.2–4,8,16,19–22 There are no randomized controlled trials that directly compare oral with topical antimicrobial therapy, and few that compare ototopicals. However, the clinical effectiveness of ototopicals, which can achieve local tissue concentrations approximately 1,000 times that of systemic administration, is persuasive, and they have fewer incidents of systemic resistance or side effects.3,8,17
Other topicals range from aminoglycosides (e.g., neomycin and gentamicin) to fluoroquinolones with or without a concomitant steroid. Ototoxicity from aminoglycosides has been associated with open middle ear spaces or prolonged use. They are to be avoided if the eardrum is not intact.3,5,19,22 Neomycin tends to be sensitizing in 5 to 18 percent of patients and can incite contact dermatitis (Figure 2).1,4,22,25,26 If acute OE fails to completely resolve, the physician should be aware that the preservatives benzalkonium chloride, thimerosal, and propylene glycol can incite local sensitization.1–4,9,15,20,24–26
Figure 2.

An auricle and ear canal affected by acute otitis externa and exhibiting a type IV hypersensitivity reaction to neomycin. Note the drainage pattern of the ear drops that have incited a cutaneous reaction on the ear lobule.
The fluoroquinolone preparations require only twice-daily dosing, and some are approved for use with a nonintact tympanic membrane. The addition of a steroid to a fluoroquinolone diminishes the symptomatic period by 0.8 days and must be balanced against the small risk of the steroid acting as a sensitizing agent.20,22 Regardless of the ototopical selected, for other than mild cases, physicians should consider seeing the patient for one further visit to verify resolution of disease and to consider cleaning any remaining canal debris.
Ten percent of acute OE is of fungal origin, but this percentage is higher in acute OE not fully responding to antibacterial drops. In this situation, the initial ototopical choice, and the possibilities of a contact sensitivity or a fungal suprainfection, must be considered.3,4,5,16 Uncomplicated fungal infections commonly manifest with whitish cotton-like strands (e.g., Candida) with or without interspersed small black or white fungal balls (e.g., Aspergillus; Figure 3). Mixed bacterial and fungal infections are common after inadequate ototopical treatment of bacterial acute OE. Most fungal infections are mild and can be treated with a 2% acetic acid and/or a 90% to 95% alcohol solution. More established disease requires topical agents such as 1% clotrimazole (Lotrimin) or tolnaftate (Tinactin).9,16,27
Figure 3.
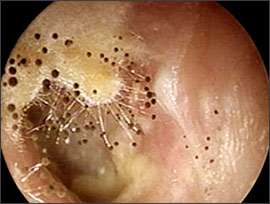
External auditory canal with Aspergillus overgrowth manifesting as a cottony matrix topped by small black balls.
Treatment of noninfectious causes of OE depends on the underlying problem. All tend to have pruritus and be of insidious onset. Generalized dermatitides often cause mild erythema and lichenification in addition to the characteristics of the underlying disease. Psoriasis and atopic dermatitis respond when therapy (commonly a systemic or topical steroid) for the underlying disease is initiated. Acne or seborrhea are managed with appropriately medicated creams or shampoos. Contact allergies respond to elimination of the offending agent, which usually can be determined from patient history, although patch testing is occasionally necessary. Chronic OE from a systemic dermatitis can be complicated by an opportunistic bacterial or fungal infection. Because such an infection is managed with an antimicrobial ototopical, persistence of the dermatitis can be misinterpreted as a treatment failure.
Complications
When initial therapy fails, physicians should consider other possible reasons, including the accuracy of the initial diagnosis (Table 2). In the unusual event of disease progression to extra-canal manifestations (e.g., auricular cellulitis, cervical adenopathy, or parotitis), addition of an oral antimicrobial is appropriate and culture is prudent.2,3,19,22 Oral antibiotics also should be considered for moderate acute OE in older patients; in patients who are immunocompromised; and in patients with diabetes, coexisting otitis media, or malignant external otitis.2,3,9,20 Malignant external otitis is an osteomyelitis of the ear canal (Figure 4). It often involves the adjacent mastoid and should be suspected when canal skin necrosis or granulation appear; the pain is disproportionate; the patient’s temperature exceeds 102.2° F (39° C); or facial paralysis, vertigo, or meningeal signs occur.2,5,9,28
TABLE 2 Considerations When Otitis Externa Fails to Respond to Initial Therapy
| Contact dermatitis (original issue or reaction to ototopical) |
| Failure to adhere to preventive measures (e.g., temporary cessation of swimming) |
| Faulty or infrequent administration of ototopical |
| Immunosuppression (requires prolonged therapy and possibly oral antibiotics) |
| Inadequate penetration of ototopical because of canal debris or narrowing |
| Malignant external otitis (requires intravenous antibiotics and debridement) |
| Misdiagnosis, including dermatologic conditions (e.g., control systemic psoriasis, seborrhea), dermatophytid reaction, cancer, self-instrumentation trauma |
| Ototopical not effective against bacteria or fungi involved (or it is a mixed bacterial and fungal problem) |
Figure 4.

Malignant external otitis with pus draining from the necrotic ear canal and underlying osteomyelitic bone. The adjacent auricle demonstrates the swelling and loss of cartilaginous architecture characteristic of chondritis.
A furuncle can occur in the ear canal de novo or as the result of acute or chronic inflammations. Cultures are taken at the time of incision and drainage, and ototopical and oral antibiotics are prescribed.
Prevention
Common precipitants of acute OE are moisture and trauma.4,5,16 One study showed that children with acute OE were more likely to have had their ears cleaned with cotton swabs, had wax removal, been swimming, or had pressure equalization tubes inserted within the previous 10 days when compared with children without acute OE.11,29 The likelihood of acute OE can be reduced through daily prophylaxis with acidifying or alcohol drops during the at-risk period (e.g., swim season, scuba diving trip), use of a hair dryer on the lowest setting with or without a head tilt to aid fluid clearance after swimming or bathing, and the avoidance of cotton swabs. The use of hypoallergenic ear canal molds (hearing aid or water exclusion varieties) with or without tight swim caps to diminish recurrent infections is controversial.30–32 Prevention is particularly important in patients who are immunocompromised; those with a systemic dermatologic condition, contact sensitivities to an ototopical, or who perspire excessively; or those for whom water sports are an avocation or common recreation.2,9,15,20
