Patients with metatarsal fractures often present to primary care settings. Initial evaluation should focus on identifying any conditions that require emergent referral, such as neurovascular compromise and open fractures. The fracture should then be characterized and treatment initiated. Referral is generally indicated for intra-articular or displaced metatarsal fractures, as well as most fractures that involve the first metatarsal or multiple metatarsals. If the midfoot is injured, care should be taken to evaluate the Lisfranc ligament. Injuries to this ligament require referral or specific treatment based on severity. Nondisplaced fractures of the metatarsal shaft usually require only a soft dressing followed by a firm, supportive shoe and progressive weight bearing. Stress fractures of the first to fourth metatarsal shafts typically heal well with rest alone and usually do not require immobilization. Avulsion fractures of the proximal fifth metatarsal tuberosity can usually be managed with a soft dressing. Proximal fifth metatarsal fractures that are distal to the tuberosity have a poorer prognosis. Radiographs should be carefully examined to distinguish these fractures from tuberosity fractures. Treatment of fractures distal to the tuberosity should be individualized based on the characteristics of the fracture and patient preference. Nondisplaced fractures of the proximal portion of metatarsals 1 through 4 can be managed acutely with a posterior splint followed by a molded, non–weight-bearing, short leg cast. If radiography reveals a normal position seven to 10 days after injury, progressive weight bearing may be started, and the cast may be removed three to four weeks later.
Metatarsal fractures represent 5 to 6 percent of fractures encountered in primary care.1,2 They range from easily managed fractures to more complicated fractures that require surgical intervention. With a basic knowledge of metatarsal injuries, primary care physicians can manage selected metatarsal fractures and identify patients who need referral. This discussion is organized into three anatomic regions—the metatarsal shaft, the proximal fifth metatarsal, and the proximal first through fourth metatarsals—each of which has unique diagnostic and therapeutic considerations. Assessment of any suspected fracture should include all of the steps listed in Table 1. Indications for referral are listed in Table 2.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| Fractures of a single metatarsal with lateral or medial displacement usually heal well without correction and may be managed like nondisplaced fractures. | C | 3,4 |
| If there is more than 3 to 4 mm displacement in a dorsal or plantar direction, or if dorsal/plantar angulation exceeds 10 degrees, reduction is usually required. | C | 4,5 |
| Most nondisplaced metatarsal shaft fractures require only a soft elastic dressing or firm, supportive shoe and progressive weight bearing. | B | 3,4,6 |
| Stress fractures of the metatarsal shaft usually heal well without immobilization and typically respond well to cessation of the causative activity for four to eight weeks. | C | 8 |
| Nondisplaced avulsion fractures of the fifth metatarsal tuberosity require symptomatic therapy only (elastic or soft bandage followed by firm shoe when tolerated). | B | 6,15,16 |
| Fractures of the proximal fifth metatarsal diaphysis require more aggressive treatment, such as early surgical fixation or prolonged casting with no weight bearing. Early surgical fixation reduces time to healing and time to return to sports. | B | 15,17–20 |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, see page 749 orhttps://www.aafp.org/afpsort.xml.
Table 1 Routine Steps in the Assessment of Possible Fractures
| Perform and document a neurovascular examination by testing capillary refill/pulses and sensation and immediately address any deficit | |
| Carefully inspect the skin for: | |
| Wounds that may indicate an open fracture | |
| Tenting of the skin over a displaced fracture | |
| Devitalized skin that may necrose | |
| Common fracture findings (e.g., swelling, ecchymosis) | |
| Less common fracture findings (e.g., deformity, fracture blisters) | |
| Palpate for point tenderness | |
| Briefly evaluate nearby joints and structures | |
| Be alert for signs and symptoms of compartment syndrome, including early symptoms such as disproportionate pain | |
Table 2 Indications for Referral in Patients with Metatarsal Fractures
| Emergent/urgent referral | |
| Associated neurologic deficit | |
| Compartment syndrome | |
| Open fracture | |
| Skin devitalized or at risk for devitalization (severe crush or shearing injuries) | |
| Vascular compromise | |
| Prompt referral* | |
| Displaced fracture of single metatarsal if: | |
| Displaced fracture of fifth metatarsal styloid | |
| Shaft fracture near the metatarsal head | |
| Unacceptable position of shaft fracture† and physician is uncomfortable performing the reduction | |
| Unsuccessful reduction attempt(s) | |
| Fifth metatarsal fracture distal to styloid in which patient is not willing to endure prolonged non–weight-bearing cast | |
| First metatarsal fracture (unless fracture is completely nondisplaced) | |
| Intra-articular fracture | |
| Lisfranc ligament injury or tenderness over Lisfranc ligament and injury cannot be ruled out | |
| Loss of acceptable position during treatment | |
| Multiple metatarsals fractured (unless nondisplaced and stable) | |
| Unsatisfactory result following treatment (including nonunion, malunion, and unacceptable chronic symptoms) | |
*—Discuss with orthopedic surgeon at time of diagnosis to determine optimal timing of referral. Some injuries should be evaluated by the surgeon on the day of diagnosis.
†—Metatarsal shaft fractures with > 3 to 4 mm displacement in the dorsal/plantar plane or > 10 degrees angulation in this plane generally require reduction.
Fractures of the Metatarsal Shaft
Because the first metatarsal is larger and more important for foot function than the other metatarsals, malalignment of a first metatarsal fracture is less well tolerated than malalignment of a lesser metatarsal. Adjacent metatarsals act as splints for a fractured metatarsal. Therefore, metatarsal fractures are usually not displaced unless there are multiple fractures or the fracture is near the metatarsal head (Figure 1). When displacement does occur, the metatarsal head usually displaces in a plantar direction as a result of traction from the flexor tendons and intrinsic muscles of the foot.
Figure 1.
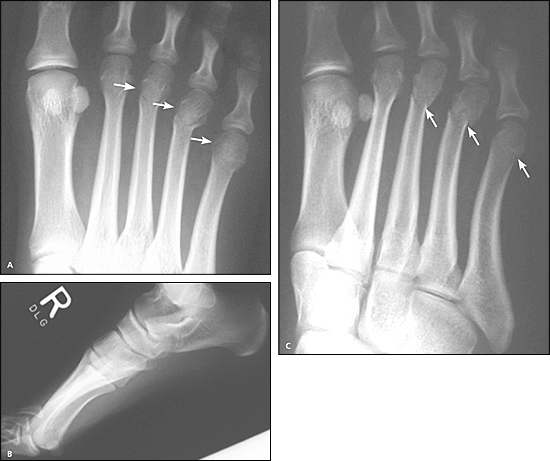
Transverse fractures of distal third to fifth metatarsal shafts. (A) Anteroposterior view. (B) Lateral view, in which the fractures are difficult to discern. (C) Oblique view, necessary to better assess position. The mild displacement of the fourth metatarsal head is facilitated by the distal location of the fracture. The fifth metatarsal fracture is extremely subtle. Clinical correlation (i.e., noting point tenderness over the fifth metatarsal neck) could be used to confirm this fracture.
ACUTE FRACTURES
Most shaft fractures are caused by direct blows or twisting forces. Patients typically present with pain, swelling, ecchymosis, and difficulty walking. Swelling is often severe, especially if the patient has not elevated the foot, and there is usually point tenderness over the fracture site. Applying an axial load to the head of a fractured metatarsal usually produces pain at the fracture site. This maneuver should not be painful in patients with soft tissue injury alone.
Radiographic Findings
Most metatarsal shaft fractures are oblique or transverse (Figure 1A). Displacement is usually minimal unless more than one metatarsal is fractured. Fracture position is best assessed using two views that lie at a 90-degree angle to each other. However, overlying shadows on the lateral view often make it difficult to see metatarsal fractures (Figure 1B). Oblique or modified lateral views are often more helpful (Figure 1C).
Acute Treatment
After conditions that require emergent referral have been ruled out (Table 2), nondisplaced metatarsal shaft fractures may be treated with a soft, padded elastic dressing or immobilized in a posterior splint. Crutches should be provided and weight bearing allowed as tolerated, with follow-up in three to five days. Elevation and icing help reduce pain and swelling and should be strongly encouraged.
Fractures of a single metatarsal shaft with lateral or medial displacement (Figure 2A) usually heal well without correction. These may be managed like nondisplaced fractures.3,4 However, if there is more than 3 to 4 mm displacement in a dorsal or plantar direction, or if dorsal/plantar angulation exceeds 10 degrees, reduction is usually required.4,5 Reduction technique and subsequent acute care are described elsewhere.4 Patients who require referral should be placed in a posterior splint and instructed not to bear weight until evaluated by a specialist.
Figure 2.

Moderately displaced oblique fracture of the fifth metatarsal shaft. (A) Anteroposterior view, showing significant (but acceptable) medial displacement. (B) Oblique view three months later demonstrating excellent callus.
Definitive Treatment
Most nondisplaced metatarsal shaft fractures require only a soft elastic dressing or firm, supportive shoe and progressive weight bearing.4,6 A postoperative shoe or cast boot may be necessary if the foot is too swollen for ordinary shoes. If the patient has significant pain despite these measures, a short leg walking cast may be worn for two to three weeks. Casted patients should be warned to seek emergency care for paraesthesia or increasing pain, which may indicate early iatrogenic compartment syndrome or a poorly fitting cast that may injure underlying soft tissues.
Radiography should be repeated one week after injury to make sure fracture position remains satisfactory, and again four to six weeks after injury to document healing.4,5 Clinical healing, defined as visible callus on radiographs (Figure 2B) and resolution of point tenderness, usually occurs by six weeks. After this occurs, protection can be discontinued. Ankle range-of-motion and calf stretching/strengthening exercises should then be initiated, especially if a cast was used. Although most metatarsal shaft fractures heal well with appropriate treatment, complications may occur (Table 3).
STRESS FRACTURES
An abrupt increase in activity or chronic overload may cause a stress fracture of the metatarsal shaft. Initially, pain occurs only with activity. Point tenderness is often present over the fracture, and axial loading of the metatarsal head may produce pain at the fracture site.7 If the injury is not allowed to heal, worsening pain, swelling, and even frank fracture may occur.
Table 3 Potential Complications of Metatarsal Fractures
| Arterial injury | |
| Compartment syndrome | |
| Complex regional pain syndrome | |
| Delayed healing and nonunion (mainly proximal fifth metatarsal fractures distal to styloid) | |
| Ischemic contracture or amputation if treatment of vascular injury or compartment syndrome is delayed | |
| Malunion (healing in unacceptable position), which may lead to: | |
| Dorsal keratosis from significant uncorrected dorsal angulation | |
| Metatarsalgia, especially with first metatarsal fractures | |
| Plantar keratosis from significant uncorrected plantar angulation of distal fragment | |
| Nerve injury | |
| Osteomyelitis (open fractures) | |
Radiographic Findings
Stress fractures are rarely visible on plain radiographs until symptoms have been present for two to six weeks.7 Over time, radiographic findings progress from subtle to more obvious. Magnetic resonance imaging or technetium bone scanning can be used to support the diagnosis.7 In patients with a typical history and appropriate physical findings, a presumptive clinical diagnosis may be made and these tests may not be necessary.
Treatment
Stress fractures of the metatarsal shaft usually heal well without immobilization, in part because of excellent blood supply. They typically respond well to cessation of the causative activity for four to eight weeks.8 If walking causes pain, several weeks of using crutches and partial weight bearing may be helpful. A non–weight-bearing, short leg cast can be used for one to three weeks in patients with severe pain. After four to eight weeks of treatment, pain typically resolves. Activities can then be gradually resumed. Recurrence is possible if activities are resumed prematurely or too rapidly. A custom orthotic may benefit certain foot structures, such as a rigid or long second metatarsal, but clinical trial evidence for injury prevention is lacking.7
Fractures of the Proximal Fifth Metatarsal
Three distinct fractures occur in the proximal fifth metatarsal. Each is treated differently, and physicians must be attentive to small differences in history, fracture location, and radiographic findings to correctly identify them.
The joint between the bases of the fourth and fifth metatarsals is a key landmark for classifying proximal fifth metatarsal fractures (Figure 3). Tuberosity (styloid) fractures always occur proximal to this joint (Figure 4). Acute fractures of the metaphyseal-diaphyseal junction (Jones fractures) extend toward this joint (Figure 5). Diaphyseal stress fractures usually occur distal to this joint (Figure 6), although stress fractures also can occur in the Jones location (Figure 5). Tuberosity fractures heal well, Jones fractures heal less well, and diaphyseal stress fractures heal poorly.
Figure 3.
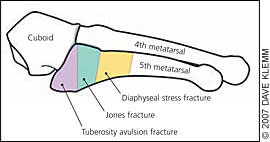
Schematic representation of fracture zones for proximal fifth metatarsal fractures.
Figure 4.
Minimally displaced avulsion fracture of the fifth metatarsal tubercle (styloid). The fracture line extends into the joint with the cuboid but not the joint with the fourth metatarsal (intermetatarsal joint).
Figure 5.

Location of typical acute fifth metatarsal diaphysis (Jones) fracture, with extension toward the intermeta-tarsal joint. The narrowing of the medullary canal suggests that this is actually a stress fracture in this location.
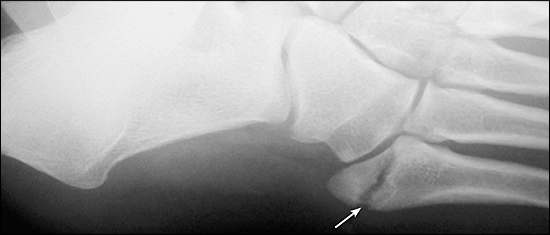
Figure 6.

Torg type II stress fracture of the metatarsal diaphysis at the characteristic location, just distal to the intermetatarsal joint.
MECHANISM OF INJURY AND PRESENTATION
Tuberosity avulsion fractures usually result from ankle inversion while the foot is in plantar flexion. The history often suggests a lateral ankle sprain, and these fractures are often missed. This can be avoided by applying the Ottawa rule for foot radiographs in ankle injuries9 (Figure 710 ).
Figure 7.
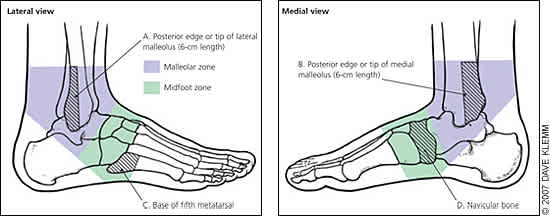
Ottawa rule for foot radiography after ankle inversion injuries. A foot radiographic series is indicated if a patient has pain in the midfoot zone and any of these findings: bone tenderness at C, bone tenderness at D, or inability to bear weight immediately and in the emergency department (or physician's office).
Adated from Wolfe MW, Uhl TL, Mattacola CG, McCluskey LC. Management of ankle sprains. Am Fam Physician 2001;63:97.
Acute diaphyseal (Jones) fractures usually result from a vertical or mediolateral force on the base of the fifth metatarsal while the patient's weight is over the lateral aspect of the plantar-flexed foot.11 This may occur during a sudden change in direction with the heel off the ground. Diaphyseal stress fractures are caused by chronic overloading, especially from jumping and pivoting activities in younger athletes.
All three fractures cause lateral foot pain and difficulty walking. Acute fractures typically have a sudden onset, with swelling and ecchymosis. Stress fractures usually cause a progressive increase in pain that is worse with activity. Recognizing the gradual onset of symptoms is key to correctly diagnosing fifth metatarsal stress fractures.
RADIOGRAPHIC FINDINGS
Examples of each proximal fifth metatarsal fracture are shown in Figures 4 through 6. Up to one fourth of tuberosity fractures may be missed on foot series.12 To avoid misdiagnosis as a sprain, an ankle series (including anteroposterior and mortise views) should be considered if point tenderness is present over the proximal fifth metatarsal and the foot series appears normal. Stress fractures may be classified using Torg's system13 (Table 414), which is helpful for establishing prognosis and selecting appropriate treatment.
Table 4 Torg's Classification System for Fractures of the Proximal Fifth Metatarsal Within 1.5 cm of the Tuberosity
| Torg classification | Radiographic appearance |
|---|---|
| Type I (early) | No intramedullary sclerosis |
| Fracture line with sharp margins and no widening | |
| Minimal cortical hypertrophy | |
| Minimal evidence of periosteal reaction to chronic stress | |
| Type II (delayed) | Fracture line that involves both cortices with associated periosteal bone union |
| Widened fracture line with adjacent radiolucency related to bone resorption | |
| Evidence of intramedullary sclerosis | |
| Type III (nonunion) | Wide fracture line |
| Periosteal new bone and radiolucency | |
| Complete obliteration of the medullary canal at the fracture site by sclerotic bone |
Reprinted from Strayer SM, Reece SG, Petrizzi MJ. Fractures of the proximal fifth meta-tarsal. Am Fam Physician 1999;59:2519.
Several radiographic findings may be confused with fractures of the fifth metatarsal. Small accessory bones near the base of the fifth metatarsal may be mistaken for avulsion fractures. Accessory bones typically have smooth, rounded edges and a hint of cortex around their entire circumference, whereas fracture fragments usually have one jagged or straight edge that lacks cortication. In early adolescence, a tendon-associated growth center (apophysis) is visible in the lateral part of the tuberosity. It has rounded, corticated edges and a horizontal orientation, whereas nearly all tuberosity fractures are transverse with sharp, uncorticated internal edges (Figure 4).
TREATMENT
Nondisplaced avulsion fractures of the tuberosity require symptomatic therapy only.6,15,16 One small randomized trial found that patients treated with a soft protective dressing returned to full function more quickly than patients treated with a short leg cast, without any adverse effects on bone healing or symptoms.16 A soft dressing can be made by wrapping the foot and ankle with cast padding and holding it in place with an elastic bandage. If the patient is too symptomatic in the soft dressing, a hard-soled shoe, brace, or cast may be used.
Regardless of the treatment selected, weight bearing is allowed as tolerated. Most of these fractures heal symptomatically in three to six weeks, with radiographic union in eight weeks.15 Referral is indicated for displaced fractures, fractures with more than a 1 to 2 mm step-off on the articular surface with the cuboid, and nonunion (Figure 8).
Figure 8.

Nonunion of a minimally displaced tubercle fracture six months after injury showing the rounded, thickened edges of the fracture line. The patient had minimal symptoms and declined further treatment.
Fractures of the proximal fifth metatarsal that are distal to the tuberosity require more aggressive treatment. This includes fractures of the metaphyseal-diaphyseal junction (Figure 5) and fractures of the diaphysis (Figure 6). Complications such as delayed union and nonunion are common. Treatment should be individualized using the guidelines in Table 5.13,15,17–20 Referral should be considered for patients who are highly active and patients who want to minimize the duration of treatment.
Table 5 Treatment of Fifth Metatarsal Diaphysis Fractures
| Fracture type | Treatment options | |
|---|---|---|
| Acute nondisplaced diaphyseal (Jones) fracture | Non–weight-bearing cast for 6 to 8 weeks13,15,17 | |
| Weight-bearing orthosis for 8 to 12 weeks18 | ||
| Consider early surgical fixation in athletes13,15,17,19 | ||
| Diaphyseal stress fracture | ||
| Type I (early) | Non–weight-bearing cast for 6 to 8 weeks13,15,17 | |
| Weight-bearing orthosis for 8 to 12 weeks18 | ||
| Consider early surgical fixation in athletes13,15,17 | ||
| Type II (delayed) | Early surgical fixation13,15,17 | |
| Non–weight-bearing cast for up to 20 weeks in selected patients13,15,17 | ||
| Type III (nonunion) | Surgical fixation13,15,17 | |
| Pulsed electromagnetic fields plus non–weight-bearing cast for up to 16 weeks20 | ||
Fractures of the Proximal First Through Fourth Metatarsals
Although fractures of the proximal first through fourth metatarsals are less common than other metatarsal fractures, they warrant special consideration because they are often associated with injury to the Lisfranc ligament complex. These crucial ligaments hold the metatarsal bases rigidly in place, maintaining the arch of the foot and anchoring the metatarsals to the rest of the body. Injuries to this ligament complex, even if subtle, can cause long-term disability and are important to detect.
In children, the physis (growth center) of the first metatarsal is located proximally, whereas the physes of metatarsals 2 through 5 are located distally. Failure to realize this can lead physicians to misinterpret a normal first metatarsal physis as a fracture.
MECHANISM OF INJURY AND PRESENTATION
Proximal metatarsal fractures are usually caused by crush injuries or direct blows. They may also result from falling forward over a plantar-flexed foot. Clinical findings and evaluation are analogous to those described above for acute shaft fractures.
In athletes, the most common mechanism for a Lisfranc injury is an axial load placed on a plantar-flexed foot (Figure 921). This mechanism should prompt strong suspicion of a Lisfranc injury. Apart from this, the mechanisms of injury and physical findings of proximal metatarsal fractures and Lisfranc injuries are similar and provide little value in distinguishing between the two. The key to detecting Lisfranc injuries is to maintain a high index of suspicion when a patient presents with pain in the area of the Lisfranc ligament. These patients should be referred or further evaluated as outlined below.
Figure 9.
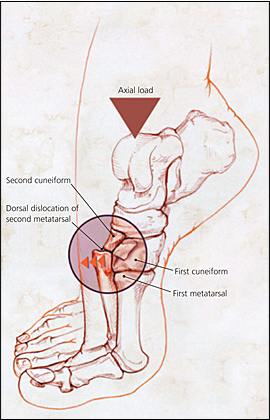
Axial load mechanism of a Lisfranc injury.
Reprinted from Burroughs KE, Reimer CD, Fields KB. Lisfranc injury of the foot: a commonly missed diagnosis. Am Fam Physician 1998;58:121.
RADIOGRAPHIC FINDINGS
Proximal metatarsal fractures are generally transverse or oblique and often multiple (Figure 10). Displacement may occur in high-force injures or when there is a concomitant injury to the Lisfranc ligament complex. To detect Lisfranc ligament injuries, it is important to carefully examine radiographs for certain clues (Figure 11). However, a standard foot series may appear normal in up to 50 percent of patients with Lisfranc injuries, even when the injury is significant.22 Therefore, patients with unexplained tenderness near the tarsometatarsal joint should be referred or further evaluated, even if standard radiographs appear normal.
Figure 10.

Nondisplaced fractures of the proximal portions of metatarsals 2 through 4 showing normal spacing between the bases of the first and second metatarsals.
Figure 11.
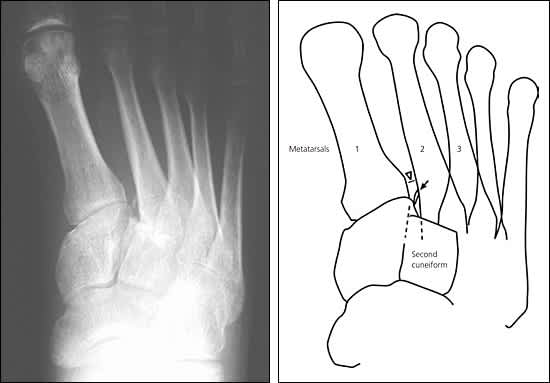
Lisfranc fracture-dislocation showing three classic findings of a Lisfranc ligament injury: (1) the widened space (diastasis) between the bases of the first and second metatarsals (white arrow head in drawing; normal spacing is visible in Figure 10); (2) the “fleck” fracture adjacent to the base of the first metatarsal (black arrow in drawing); and (3) loss of alignment of the medial edge of the proximal second metatarsal with the medial edge of the second cuneiform (dashed lines in drawing).
Further evaluation begins with weight-bearing antero-posterior and lateral radiographs. With significant disruption of the Lisfranc ligament (stage II or III), the anteroposterior view demonstrates widening of the space between the first and second metatarsal heads (diastasis)22 (Figure 11). Arch height is lost on the lateral view in stage III injuries.
A stage I injury should be suspected if weight-bearing views are normal but the patient has tenderness over the tarsometatarsal area and pain with activity.22 In this setting, a positive bone scintigram appears to be extremely accurate for establishing the diagnosis (sensitivity of 100 percent in a small study with eight patients).22 When a stage I injury is suspected, it is important to pursue the diagnosis with a bone scintigram or to refer the patient, because this injury requires specific treatment (non–weight-bearing cast for six weeks).22
TREATMENT
Provided an injury to the Lisfranc ligament is not suspected and there is no other indication for referral (Table 2), nondisplaced proximal fractures of metatarsals 1 through 4 can be managed acutely with a posterior splint and no weight bearing. In three to five days, a molded, non–weight-bearing, short leg cast may be applied. Seven to 10 days after injury, radiographs should be obtained through the cast to check fracture position. If position is still good, the cast should be worn for three to four more weeks with progressive weight bearing. Range-of-motion, stretching, and strengthening exercises should be initiated on cast removal.
If a stage I Lisfranc injury cannot be ruled out, it may be prudent to treat with a non–weight-bearing cast for a full six weeks or to obtain orthopedic consultation. After treatment, certain activities may be limited by pain, especially if the anatomic position was not restored or a Lisfranc injury was missed. Other potential complications are listed in Table 3.
