to the editor: The prevalence of congenital heart disease (CHD) in the adult population has risen secondary to advances in diagnostic and therapeutic techniques. The population sizes of adult and pediatric patients with CHD are comparable.1 Many adult patients have coarctation of the aorta (COA) caused by low perioperative morbidity and mortality and excellent long-term survival after surgical repair in childhood. As a direct result, primary care physicians should be comfortable assessing such patients for recurrence of the condition, which has been reported to be as high as 3 percent.2 We would like to present a case in which a careful and systematic physical examination yielded an alternative diagnosis in a patient whose hypertension was long believed to be secondary to cocaine abuse.
A 59-year-old man presented to the emergency department complaining of intermittent chest pain associated with cocaine use. He reported a history of valve surgery as a child, but was unable to provide details. Inspection of the chest wall revealed a midaxillary scar at the level of the 5th or 6th rib. Cardiac auscultation was normal. Vascular examination revealed a significant radio-femoral delay. Palpation of the back revealed pulsatile intercostal arteries at multiple levels.
Coronary angiography and aortography was pursued to evaluate for coronary artery disease and COA. Upon gaining access to the femoral artery, a large discrepancy in blood pressure compared with the brachial cuff pressure was noted (92/70 mm Hg and 180/76 mm Hg, respectively). Coronary angiography revealed normal arteries; however, aortography was significant for a 90 percent stenosis immediately distal to the left subclavian artery (see accompanying figure). A gradient across the lesion of 100 mm Hg was found. At the level of the stenosis, there were fluoroscopic findings suggestive of previous surgical manipulation.
Figure 1.
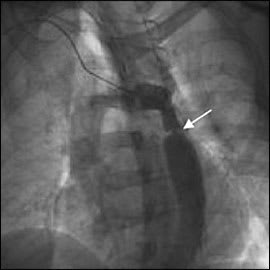
Aortography indicating coarctation of the aorta (arrow).
This case serves as a reminder that hypertension has numerous etiologies, some of which are uncommon. Although cocaine toxicity undoubtedly contributed to the patient's symptoms, our examination uncovered the recurrence of a hemodynamically significant congenital abnormality.
A heightened level of suspicion for COA is essential when a greater than 20 mm Hg difference between systolic arm and leg blood pressures is present.3 Other clinical findings suggestive of COA include palpable intercostal pulses caused by collateral flow; chest radiographs demonstrating rib notching; and scars from childhood surgery.
Survivors of COA repair have increased morbidity and mortality as adults and require close follow-up.3 Primary care physicians are a critical component of this process because prompt detection of recurrence may help improve health outcomes in patients with recurrent COA.
