A 73-year-old woman presented with dizziness, uncomfortable chest pressure that worsened during exertion, and headache; her symptoms began two days earlier. The patient had a history of hypertension and atrial fibrillation. She had a cerebral vascular accident 11 years earlier that led to visual and motor sequelae. Since then, she had been taking 200 mg of amiodarone (Pacerone), 20 mg of enalapril (Vasotec), and 150 mg of aspirin daily. Physical examination revealed bradycardia (42 beats per minute) as well as asymptomatic, blue-gray to purple facial pigmentation (Figure 1). Thyroid, lung, liver, and kidney function and autoimmunity test results were normal. At the follow-up visit, the patient's heart rate was normal without the use of amiodarone, but her skin remained discolored.
Figure 1.

Question
Based on the patient's history and physical examination, which one of the following is the most likely diagnosis?
A. Amiodarone-induced hyperpigmentation.
B. Chloasma.
C. Erythema dyschromicum perstans.
D. Localized discoid lupus erythematosus.
E. Riehl melanosis.
Discussion
The answer is A: amiodarone-induced hyperpigmentation. Amiodarone is an iodine-rich medication that is widely used to manage cardiac arrhythmias. It has numerous adverse effects, such as toxicity of the lungs, thyroid, liver, eyes, and nerves. A blue-gray discoloration of the skin is an uncommon adverse effect caused by the ultraviolet accumulation of lipofuscin in dermal macrophages. The appearance of the discoloration depends on the dosage of amiodarone and duration of use, and may regress upon cessation of the treatment.1 Biopsy confirms skin impregnation of iodine with deposition of brown pigment within dermal microphages (Figure 2).
Figure 2.
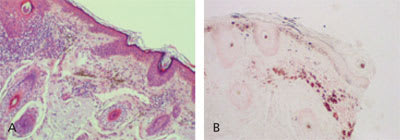
Biopsy findings confirming skin impregnation of iodine with deposition of brown pigment within dermal microphages. (A) Hematoxylin stain. (B) Fontana-Masson stain.
Chloasma, or melasma, is an acquired hypermelanosis that is common during pregnancy. It is characterized by irregular, light brown to gray-brown macules involving the face, particularly the cheeks, forehead, nose, upper lip, and chin. Histologic findings include increased activity and numbers of melanocytes, with sparse or absent inflammation.2
Erythema dyschromicum perstans (ashy dermatosis) is an acquired, benign condition characterized by asymptomatic, slate-gray to violet or blue macules. The etiology of the condition is unknown. Its histologic pattern is relatively nonspecific with pigment incontinence, peri-vascular lymphohistiocytic infiltrate, and an immune-associated antigen expression in keratinocytes.3
Localized discoid lupus erythematosus occurs on sun-exposed areas of the face, particularly the bridge of the nose, lower eyelids, lower lip, and ears. Initially, active lesions are red or violet, with lighter scaly centers and darker outer rings. Antibodies against double-stranded DNA are almost always absent. Histopathologic alterations include atrophy of the epidermis, hyperkeratosis, follicular plugging, vacuolar degeneration of the basal cell layer with marked melanin deposits in the upper dermis following basal cell damage, and heavy peri-adnexal mononuclear cell infiltration.4
Riehl melanosis is a spotty, brown-gray facial pigmentation most pronounced on the forehead and the zygomatic and temporal regions. It occurs in persons with a history of exposure to cosmetics. Severe cases may appear black, purple, or blue-black. Histologic findings include a lymphohistiocytic infiltrate in the upper dermis.5
Selected Differential Diagnosis of Facial Hyperpigmentation
| Condition | Characteristics |
|---|---|
| Amiodarone-induced hyperpigmentation | Blue-gray facial pigmentation with accumulation of lipofuscin in dermal macrophages |
| Chloasma | Irregular, light brown to gray-brown macules with increased activity and numbers of melanocytes with sparse or absent inflammation |
| Erythema dyschromicum perstans | Slate-gray to violet or blue macules with perivascular lymphohistiocytic infiltrate; pigment incontinence and immune-associated antigen expression in keratinocytes |
| Localized discoid lupus erythematosus | Erythematous lesions with vacuolar degeneration of the basal cell layer and marked melanin deposits in the upper dermis following basal cell damage; atrophy of the epidermis; hyperkeratosis; follicular plugging |
| Riehl melanosis | Spotty brown-gray facial pigmentation with lymphohistiocytic infiltrate in the upper dermis |
