Deviations from a normal age-appropriate gait pattern can be caused by a wide variety of conditions. In most children, limping is caused by a mild, self-limiting event, such as a contusion, strain, or sprain. In some cases, however, a limp can be a sign of a serious or even life-threatening condition. Delays in diagnosis and treatment can result in significant morbidity and mortality. Examination of a limping child should begin with a thorough history, focusing on the presence of pain, any history of trauma, and any associated systemic symptoms. The presence of fever, night sweats, weight loss, and anorexia suggests the possibility of infection, inflammation, or malignancy. Physical examination should focus on identifying the type of limp and localizing the site of pathology by direct palpation and by examining the range of motion of individual joints. Localized tenderness may indicate contusions, fractures, osteomyelitis, or malignancy. A palpable mass raises the concern of malignancy. The child should be carefully examined because nonmusculoskeletal conditions can cause limping. Based on the most probable diagnoses suggested by the history and physical examination, the appropriate use of laboratory tests and imaging studies can help confirm the diagnosis.
A normal mature gait cycle consists of the stance phase, during which the foot is in contact with the ground, and the swing phase, during which the foot is in the air. The stance phase is further divided into three major periods: the initial double-limb support, followed by the single-limb stance, then another period of double-limb support.1
The gait undergoes orderly stages of development. Walking velocity, step length, and the duration of the single-limb stance increase with age, whereas the number of steps taken per minute decreases. A mature gait pattern is well established by three years of age, and the gait of a seven-year-old child closely approximates that of an adult.2
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
The following clinical features are more predictive of septic arthritis than of transient synovitis:
| C | 5 |
| The initial imaging modality for a limping child who has focal findings on physical examination is anteroposterior and lateral radiography of the involved site. | C | 29 |
| The initial imaging modality for a limping child who has no focal findings on physical examination is radiography of both lower extremities. | C | 29 |
| Ultrasonography is recommended over plain-film radiography for detecting hip effusion. | C | 32 |
| A bone scan is recommended for detecting underlying pathology when other imaging modalities have failed. | C | 33–36 |
| When infection, inflammatory arthritis, or malignancy is suspected, a complete blood count with differential and measurement of ESR and CRP level should be obtained. | C | 23–25, 33, 46 |
CRP = C-reactive protein; ESR = erythrocyte sedimentation rate.
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.xml.
Abnormal Gait
Abnormal gait can be antalgic or nonantalgic. An antalgic gait, which is characterized by a shortening of the stance phase, is a compensatory mechanism adopted to prevent pain in the affected leg. Because there is decreased contact between the affected leg and the ground, a child with such a gait may not report pain. There are several different types of nonantalgic gait (Figure 1); most of these do not require urgent evaluation and treatment.
Figure 1. Diagnosis of Children with a Nonantalgic Gait
Diagnostic approach to a child with a nonantalgic gait. (CTEV = congenital talipes equinovarus; DDH = developmental dysplasia of the hip.)
The incidence of limping in children is unknown. One study of children presenting to an emergency department for an acute atraumatic limp reported a rate of 1.8 per 1,000 children younger than 14 years, a male-to-female ratio of 1.7:1, and a median age of 4.4 years.3 The limb involved (right or left) was nearly equal, and 80 percent of the children reported pain. Transient synovitis was the most common diagnosis.
Diagnosis
Limping in a child can have a variety of etiologies (Table 1). A detailed history and physical examination, in addition to appropriate laboratory tests and imaging, are essential for making a correct diagnosis (Figure 1 and Figure 24–6).
Table 1. Differential Diagnosis of Limping in Children
| Bone conditions | |
| Benign neoplasm | |
| Osteoblastoma | |
| Osteoid osteoma | |
| Congenital condition | |
| Clubfoot | |
| Congenitally short femur | |
| Developmental dysplasia of the hip | |
| Developmental condition | |
| Legg disease | |
| Slipped capital femoral epiphysis | |
| Infection | |
| Osteomyelitis | |
| Limb length discrepancy | |
| Malignant neoplasm | |
| Ewing sarcoma | |
| Leukemia | |
| Osteosarcoma | |
| Osteonecrosis | |
| Sickle cell disease | |
| Overuse injury | |
| Osteochondritis dissecans | |
| Stress fracture | |
| Trauma | |
| Child abuse | |
| Fracture (toddler’s fracture) | |
| Intra-abdominal conditions | |
| Appendicitis | |
| Neuroblastoma | |
| Psoas abscess | |
| Intra-articular conditions | |
| Congenital condition | |
| Discoid lateral meniscus | |
| Hemarthrosis | |
| Hemophilia | |
| Trauma | |
| Infection | |
| Gonorrhea | |
| Lyme disease | |
| Septic arthritis | |
| Inflammation | |
| Acute rheumatic fever | |
| Juvenile rheumatoid arthritis | |
| Reactive arthritis | |
| Systemic lupus erythematosus | |
| Transient synovitis | |
| Trauma | |
| Intra-articular injury | |
| Neuromuscular conditions | |
| Cerebral palsy | |
| Meningitis | |
| Muscular dystrophy | |
| Myelomeningocele | |
| Soft tissue conditions | |
| Congenital condition | |
| Idiopathic tight Achilles tendon | |
| Infection | |
| Cellulitis | |
| Pyomyositis or viral myositis | |
| Soft tissue abscess | |
| Overuse injury | |
| Chondromalacia patellae | |
| Jumper’s knee | |
| Osgood-Schlatter disease | |
| Sever disease | |
| Trauma | |
| Child abuse | |
| Foreign body | |
| Sprains and strains | |
| Spinal conditions | |
| Diskitis | |
| Spinal cord tumors | |
| Vertebral osteomyelitis | |
Figure 2. Diagnosis of Children with an Antalgic Gait
Diagnostic approach to a child with an antalgic gait. (CBC = complete blood count; CRP = C-reactive protein; ESR = erythrocyte sedimentation rate; MRI = magnetic resonance imaging; WBC = white blood cells.)
Information from references 4 through 6.
HISTORY
A thorough history should be obtained from the child and parents. In some cases, such as when child abuse is suspected, the child and parents should be interviewed separately. The initial history should be structured to determine the presence and nature of pain, history of trauma, and associated systemic signs (Table 2). Isolated musculoskeletal pain in the absence of other signs or symptoms is almost never a presenting symptom in children with chronic arthritis.7 Malignant bone tumors can present with intermittent pain at rest, which often misleads physicians into believing the condition is temporary and benign.8 The presence of systemic symptoms such as fever, weight loss, night sweats, and anorexia is highly suspicious for infection, inflammation, or malignancy.
Table 2. Findings from Patient History That Suggest Possible Causes of Limping in Children
| Sign or symptom | Possible cause |
|---|---|
| Acute onset of pain | Fracture |
| Associated abdominal pain | Acute abdomen |
| Neuroblastoma | |
| Psoas abscess | |
| Associated back pain | Diskitis |
| Spinal cord tumors | |
| Vertebral osteomyelitis | |
| Associated fever, anorexia, weight loss, night sweats | Malignancy |
| Osteomyelitis | |
| Rheumatologic disorder | |
| Septic arthritis | |
| Associated neck pain, photophobia, or fever | Meningitis |
| Burning pain | Nerve involvement |
| Constant pain | Infection |
| Malignancy | |
| Focal pain | Fracture |
| Infection | |
| Malignancy | |
| Gradually worsening pain | Malignancy |
| Osteomyelitis | |
| Rheumatologic disorder | |
| Stress fracture | |
| History of bleeding disorder | Hemarthrosis |
| History of insect bite | Lyme disease |
| History of preceding diarrhea | Reactive arthritis |
| History of preceding pharyngitis | Acute rheumatic fever |
| History of trauma | Fracture |
| Intra-articular injury | |
| Soft tissue injury | |
| Intermittent pain at rest | Malignancy |
| Migratory polyarthralgia | Acute rheumatic fever |
| Gonococcal arthritis | |
| Morning stiffness | Rheumatologic disorder |
| Stress fracture | |
| Pain improves with activity | Rheumatologic disorder |
| Pain worsens with activity | Overuse injury |
| Stress fracture | |
| Pain in morning or after inactivity | Rheumatologic disorder |
| Pain at night | Malignancy |
| Radiating pain | Nerve or spinal cord involvement |
| Sexually active child | Gonococcal arthritis |
| Reactive arthritis |
PHYSICAL EXAMINATION
The main goals of the physical examination are to identify the type of limp and, if possible, to localize the site of pain (Table 3).
Table 3. Findings from Physical Examination That Suggest Possible Causes of Limping in Children
| Finding | Possible cause |
|---|---|
| Abdominal mass | Neuroblastoma Psoas abscess |
| Abdominal tenderness | Acute abdomen |
| Asymmetrical gluteal and thigh skin folds | Developmental dysplasia of the hip |
| Calf hypertrophy | Muscular dystrophy |
| Conjunctivitis, enthesitis, oligoarthritis, urethritis | Reactive arthritis |
| Erythema chronicum migrans | Lyme disease |
| Erythema marginatum | Rheumatic fever |
| External hip rotation with hip flexion | Slipped capital femoral epiphysis |
| Galeazzi sign | Limb-length discrepancy |
| Hepatomegaly, lymph-adenopathy, splenomegaly | Malignancy Rheumatologic disorder |
| Hip joint flexed, abducted, externally rotated | Hip joint effusion (position maximizes joint volume and relieves pain) |
| Joint swelling | Hemophilia Inflammatory arthritis Reactive arthritis Septic arthritis |
| Localized bony tenderness | Contusion Fracture Malignancy Osteomyelitis |
| Loss of hip abduction | Developmental dysplasia of the hip |
| Loss of hip internal rotation | Legg disease Slipped capital femoral epiphysis |
| Malar rash | Systemic lupus erythematosus |
| Muscular arthropathy | Disuse muscular atrophy Neurologic disorder |
| Neck pain and stiffness, Brudzinski and Kernig signs | Meningitis |
| Non-weight bearing, painful limitation of range of motion | Septic arthritis |
| Obesity | Slipped capital femoral epiphysis |
| Overlying warmth or redness | Inflammatory arthritis Osteomyelitis Septic arthritis |
| Painless, nonpruritic maculopapular or vesicular skin rash, polyarthritis, tenosynovitis | Gonococcal arthritis |
| Palpable bony mass | Malignancy |
| Positive Patrick (FABER) test | Sacroiliac joint pathology |
| Positive pelvic compression test | Sacroiliac joint pathology |
| Positive Trendelenburg test | Developmental dysplasia of the hip Weak hip abductors |
| Psoas sign | Appendicitis Psoas abscess |
Limp Type. Gait is best examined by having the child walk and run while he or she is distracted. Each limb segment should be observed systematically through several gait cycles. The stance and swing phases should be compared in both legs, and the range of motion of each joint should be evaluated. Upper body posturing and frontal plane abnormalities (e.g., scoliosis, varus and valgus deformities) should be noted. Differentiating between antalgic and nonantalgic gait and identifying the specific type of nonantalgic gait (Figure 1) help narrow the differential diagnosis.
Site of Pathology. The child should be unclothed during the examination. The resting limb position should be noted, and both sides should be compared for symmetry; areas of erythema, swelling, and deformity should be noted. The legs should then be palpated to localize the point of maximal tenderness and to detect any masses. Range of motion should be assessed in each joint, especially the hip (Figure 3 and Figure 49). Joints adjacent to the painful one should be examined to rule out referred pain. This is especially important for hip conditions, which can present as knee or lateral thigh pain,4 leading to delayed diagnosis.10
Figure 3.

Internal rotation of the hip is measured by placing the child in the prone position with knees flexed 90 degrees and rotating the feet outward. Loss of internal rotation is a sensitive indicator of intraarticular hip pathology and is common in children with Legg disease and slipped capital femoral epiphysis.
Figure 4.

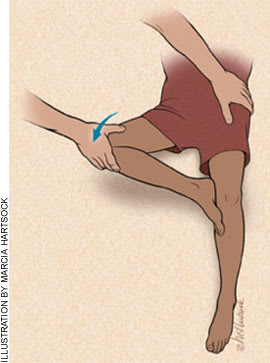
Hip abduction is measured by placing the child in the supine position with hips and knees flexed and the toes placed together. To measure abduction, both knees are allowed to fall outward. Limited hip abduction, as in this child’s left hip, occurs in children with developmental dysplasia of the hip.
Reprinted with permission from Storer SK, Skaggs DL. Developmental dysplasia of the hip. Am Fam Physician. 2006;74(8):1313.
Tests: The Trendelenburg test can be used to identify conditions that cause weakness in the hip abductors. The child stands on the affected limb and lifts the unaffected limb from the floor. In a positive test, the pelvis fails to stay level and drops down toward the unaffected side.
The Galeazzi sign can signal conditions that cause a leg-length discrepancy. The child should lie in the supine position with the hips and knees flexed. The test is positive if the knee on the affected side is lower than that on the normal side (Figure 5).
Figure 5.

Positive Galeazzi sign. The child is placed in the supine position with the hips and knees flexed. In a positive test, the knee on the affected side is lower than the normal side. This can occur in patients with any condition that causes a leg-length discrepancy, such as developmental dysplasia of the hip, Legg disease, or femoral shortening.
The Patrick test (also called the FABER test; Figure 6) can indicate pathology of the sacroiliac joint. With the child in the supine position, the examiner flexes, abducts, and externally rotates the hip joint. In a positive test, pain occurs in the sacroiliac joint.
Figure 6.
The Patrick (FABER) test. Note how the examiner has flexed, abducted, and externally rotated the child’s right hip.
The pelvic compression test also can indicate the presence of sacroiliac joint pathology. With the child in the supine position, the examiner compresses the iliac wings toward each other. Pain with this maneuver indicates sacroiliac joint pathology.
The psoas sign can signal a psoas abscess or appendicitis. With the child lying on his or her side, the hip is passively extended. Pain with hip extension indicates a positive test.
Special attention should be paid to performing a thorough spinal, pelvic, neurologic, abdominal, and genitourinary examination. Conditions affecting these systems are associated with limping (Table 1).
LABORATORY TESTS
A complete blood count with differential and measurement of the erythrocyte sedimentation rate (ESR) and C-reactive protein (CRP) levels should be obtained when infection, inflammatory arthritis, or malignancy is suspected. If septic arthritis is suspected, joint fluid should be aspirated urgently for Gram stain, culture, and cell count. Blood cultures should be obtained when infection is suspected, and bone cultures should be obtained in patients with suspected osteomyelitis. The role of specific laboratory testing is summarized in Table 4.11–28
Table 4. Laboratory Tests for Diagnosis in a Limping Child
| Test | Condition | Expected finding | Comments |
|---|---|---|---|
| ANA | SLE | Positive | Present in 94 percent of children with SLE11; a negative ANA test virtually rules out SLE.12 |
| The test’s predictive value is low in most nonspecialty settings; most positive results do not indicate SLE.13 | |||
| Ten to 40 percent of healthy children can have a positive test.12,14 | |||
| Test can be positive in patients with other medical conditions (e.g., infection, malignancy, other autoimmune conditions).13,15 | |||
| A titer between 1:160 and 1:320 offers the best combination of high sensitivity and high specificity.12 | |||
| A positive test by itself is not diagnostic for SLE; three additional criteria must be present.16 | |||
| Test is of no diagnostic utility in ruling in or ruling out juvenile rheumatoid arthritis.17 | |||
| ASO | Acute rheumatic fever | Increased ASO titers | Indicates true infection rather than carriage. |
| Elevated ASO titers are found in up to 80 percent of patients with acute rheumatic fever.18 | |||
| Sensitivity can be further increased by testing for additional antibodies.18 | |||
| Blood culture | Infection | Positive | Test is positive in 30 to 60 percent of patients with osteomyelitis19 and in 40 to 50 percent of patients with septic arthritis.20 |
| Bone culture | Osteomyelitis | Positive | Test is positive in 48 to 85 percent of patients with osteomyelitis.19 |
| Staphylococcus aureus is the most common pathogen isolated.19 | |||
| CBC | Infection | Increased WBCs and platelets | WBC count is neither sensitive nor specific for infection, inflammation, or malignancy. |
| Inflammation | Increased WBCs and platelets | Blast cells, lymphocytosis, and neutropenia may be seen in patients with leukemia.21 | |
| Malignancy | Cytopenia22 | Cytopenia may occur in patients with SLE.11 | |
| Coagulation profile | Known hemophilia or hemorrhagic effusion | Increased activated partial thromboplastin time | — |
| CRP | Infection | Increased CRP levels | Test is neither sensitive nor specific for infection, inflammation, or malignancy. |
| Inflammation | Increased CRP levels | The negative probability of septic arthritis is 87 percent when CRP level is > 1 mg per dL (10 mg per L).23 | |
| Malignancy | Increased CRP levels | In patients with osteomyelitis and septic arthritis, CRP levels should rapidly normalize after initiation of therapy. A persistently elevated CRP level after the initiation of antibiotics indicates a poor response to therapy.24,25 | |
| ESR | Infection | Increased ESR | Test is neither sensitive nor specific for infection, inflammation, or malignancy. |
| Inflammation | Increased ESR | The negative probability of septic arthritis is 85 percent when ESR is > 25 mm per hour.23 | |
| Malignancy | Increased ESR | A low or normal platelet count in the presence of an elevated ESR suggests malignancy.22 | |
| Lyme titer | Lyme disease | Positive | All children who live in or have recently traveled to an area endemic for Lyme disease should be tested.26 |
| Synovial fluid analysis | Septic arthritis | Turbid synovial fluid; WBC count > 50,000 to 100,000 per mm3; PMNs > 75 percent27 | — |
| Transient synovitis | Clear yellow synovial fluid; WBC count 5,000 to 15,000 per mm3; PMNs < 25 percent27 | ||
| Synovial fluid culture | Septic arthritis | Positive | Test is positive in 50 to 80 percent of patients with septic arthritis.20 |
| Transient synovitis | Negative | S. aureus is the most common pathogen isolated in patients with septic arthritis.27 | |
| Throat culture | Acute rheumatic fever | Group A hemolytic streptococci | Positive in only 10 to 33 percent of patients with acute rheumatic fever.18 |
| Urethral, cervical, pharyngeal, and rectal cultures | Gonococcal arthritis | Neisseria gonorrhoeae | — |
| Urethral and stool cultures | Reactive arthritis | Chlamydia in urethral cultures28; Salmonella, Shigella, Yersinia, and Campylobacter in stool cultures28 | — |
ANA = antinuclear antibodies; ASO = antistreptolysin O titer; CBC = complete blood count; CRP = C-reactive protein; ESR = erythrocyte sedimentation rate; PMN = polymorphonuclear neutrophils; SLE = systemic lupus erythematosus; WBC = white blood cell.
IMAGING
Imaging should begin with standard orthogonal radiographs of the area of concern.29 When imaging the hip, frog-leg lateral radiographs should always be obtained (Figure 7). The exception is in patients with suspected acute slipped capital femoral epiphysis, in whom a true lateral view of the hip should be obtained because a frog-leg view can cause exacerbation of the slip.30 In children with a nonfocal clinical examination, and in those who are too young to localize pain or give a reliable history, the entire lower legs should be imaged.29 Initial radiographs may be normal in children with stress fractures, toddler’s fracture,31 Legg disease, osteomyelitis, or septic arthritis.
Figure 7.

Frog-leg lateral radiograph of a patient with slipped capital femoral epiphysis. Note the slip in the patient’s right hip (arrow) compared with the normal left hip.
Ultrasonography is highly sensitive for detecting effusion in the hip joint, but it cannot differentiate between sterile, purulent, or hemorrhagic fluid accumulations.32 If an effusion is seen in the hip joint and the clinical suspicion for septic arthritis is high, urgent ultrasound-guided aspiration should be performed, and the joint fluid should be sent for Gram stain, cell count, and culture. In such circumstances, aspiration must not be delayed.33 If ultrasonography is not available, aspiration of the hip can be performed under fluoroscopic guidance. If neither of these imaging modalities is available, blind needle aspiration of the hip joint can be performed, but it carries a risk of injury to the femoral and obturator neurovascular structures, and the proper location of the needle cannot be confirmed. Blind needle aspiration should be performed only by experienced physicians when neither sonographic nor fluoroscopic guidance is available.
Bone scintigraphy is an excellent test for evaluating a limping child when the history, physical examination, and radiographic and ultrasound findings fail to localize the pathology.33–36 Bone scanning allows the entire skeleton to be imaged simultaneously and is useful for detecting occult fractures, stress fractures, osteomyelitis, tumors, and metastatic lesions. Although it has a high sensitivity, this imaging modality lacks specificity.
Computed tomography (CT) is indicated when cortical bone must be visualized.33 Magnetic resonance imaging (MRI) gives excellent visualization of joints, soft tissues, cartilage, and medullary bone.33 Unlike bone scanning, MRI has both high sensitivity and specificity. It is especially useful for confirming osteomyelitis37,38 (Figure 8), delineating the extent of malignancies, identifying stress fractures,39,40 and diagnosing early Legg disease.41–43 Fifteen to 63 percent of patients with slipped capital femoral epiphysis have involvement of the contralateral hip,44 and MRI is useful for diagnosing “pre-slips” in these patients.45
Figure 8.

Magnetic resonance image of a patient with osteomyelitis. Note the signal change within the bone marrow consistent with osteomyelitis (long arrow) and a subperiosteal abscess (small arrow). This patient had normal plain radiographs.
Common Diagnostic Dilemmas
SEPTIC ARTHRITIS VS. TRANSIENT SYNOVITIS OF THE HIP
Children with transient synovitis often are afebrile, appear nontoxic, and have less acute pain and range-of-motion restriction in the hip than those with septic arthritis, who typically appear toxic and have pain with movement of the joint in any direction. However, differentiating the two conditions can be difficult. A recent study used an oral temperature of greater than 101.3°F (38.5°C), refusal to bear weight on the affected leg, ESR greater than 40 mm per hour, peripheral white blood cell count of more than 12,000 cells per mm3 (12.0 × 109 cells per L), and a CRP level greater than 2.0 mg per dL (20.0 mg per L) as predictors to distinguish between the two conditions.5 The probability of having septic arthritis was 37 percent with one predictor present, 63 percent with two, 83 percent with three, 93 percent with four, and 98 percent with all five predictors. Hip aspiration is the gold standard for diagnosing septic arthritis and should be performed whenever septic arthritis is suspected, because the sequelae of a missed or late diagnosis can be severe.46
DISKITIS VS. VERTEBRAL OSTEOMYELITIS
Children with diskitis or vertebral osteomyelitis can present with a fever, back pain, or a limp, or they may refuse to walk. Although fever is present in both conditions, it is much more common, usually higher, and of longer duration in children with vertebral osteomyelitis.6 Children with diskitis usually do not appear ill, whereas those with vertebral osteomyelitis have a toxic appearance. In addition, diskitis involves the lumbar region almost exclusively, whereas vertebral osteomyelitis can involve any part of the spine. Radiographs of children with diskitis may show disk space narrowing and variable degrees of destruction of adjacent vertebral end plates; in children with vertebral osteomyelitis, localized rarefaction of one vertebral body and bony destruction may be seen. MRI is the diagnostic study of choice in children with suspected vertebral osteomyelitis.
MALIGNANCIES VS. RHEUMATOLOGIC DISEASES
Children with malignancies or rheumatologic conditions can have overlapping clinical features, such as musculoskeletal pain, fever, fatigue, weight loss, heaptomegaly, and arthritis.22 Nonarticular bone pain, back pain, bone tenderness, severe constitutional symptoms, night sweats, ecchymoses, bruising, abnormal neurologic signs, and abnormal masses are suggestive of malignancy.22 An elevated ESR in the presence of a normal or low platelet count also is worrisome for malignancy.22 One study found that in children presenting with unexplained musculoskeletal symptoms, a history of nighttime pain and the presence of a low white blood cell count and a low to normal platelet count has a sensitivity of 100 percent and a specificity of 85 percent for the diagnosis of acute lymphocytic leukemia.47
PSOAS ABSCESS VS. SEPTIC ARTHRITIS
Children with a psoas abscess commonly present with a limp and pain around the hip. Differentiating a psoas abscess from septic arthritis of the hip can be challenging. Patients with a psoas abscess may have a palpable abdominal mass and a positive psoas sign. Because of the proximity of the psoas abscess to the spine and the peripheral nerves, scoliosis, sciatica, and femoral nerve neuropathy may be present.48 Unlike children with septic arthritis, in whom range of motion is painfully limited in all directions, flexing the hip of a child with a psoas abscess relieves the pain and allows painless internal and external rotation of the hip. Plain-film radiography in children with psoas abscess may show obscuration of the sacroiliac joint; CT or MRI can be used to confirm the diagnosis.
