A 38-year-old woman presented with discomfort in her right shoulder and upper midback, which had persisted for two weeks. The discomfort was nonradiating and dull, and did not interfere with her daily activities, strength, or range of motion. The patient had occasional discomfort in her chest when sleeping on her right side or back; however, she denied having dyspnea, orthopnea, paroxysmal nocturnal dyspnea, cough, or other upper respiratory symptoms. She did not use tobacco and had no exposure to harsh occupational chemicals. She had a history of hypertension, which was controlled with medication. No notable surgical or family history was reported.
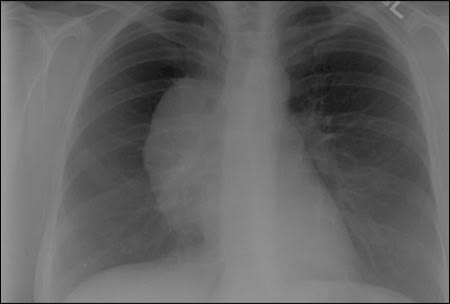
On examination, the patient's vital signs were normal. Her heart rate and rhythm were regular, and her lungs were clear on auscultation without wheezing or rhonchi. However, she had intense chest discomfort with deep inspiration. Musculoskeletal examination revealed no point tenderness in the anterior or posterior aspects of the right shoulder, and she exhibited good range of motion without joint crepitus. Despite normal physical examination findings, the discomfort with inspiration warranted further investigation, and chest radiography was performed, revealing an anterior mediastinal mass (see accompanying figure).
Question
Based on the patient's history, physical examination, and radiography findings, which one of the following is the most likely diagnosis?
A. Lymphoma.
B. Pneumothorax.
C. Teratoma.
D. Thymoma.
E. Thyroid goiter.
Discussion
The answer is C: teratoma. Benign, mature teratomas are most common in adults 20 to 40 years of age, with equal prevalence between men and women.1,2 They are germ cell tumors that arise from embryonic tissue that did not migrate during development.2
Approximately 50 percent of all mediastinal tumors occur in the anterior compartment of the mediastinum, between the sternum and the heart. Although teratomas are uncommon, they account for 10 to 20 percent of mediastinal tumors.3 Teratomas are slow growing and usually asymptomatic.2–4 However, symptoms may include chest pain, cough, or dyspnea secondary to compression of surrounding structures.2,4 A rare, but pathognomonic, symptom is trichoptysis (sputum consisting of hair).2 Teratomas are usually found incidentally on chest radiography. Teratomas are characteristically large, round, and lobulated with sharp margins.3–6 Calcification of the mass is the most characteristic radiography finding.5 Treatment of a teratoma includes surgical excision and has a five-year survival rate of 100 percent.1–8
Lymphomas are malignant tumors found in the anterior mediastinum. They are most common between 20 and 40 years of age2 and can be classified as Hodgkin or non-Hodgkin lymphoma. Symptoms may arise secondary to compression or involvement of surrounding structures. Weight loss, fever, and night sweats may also occur.2 Although results of radiography may be abnormal, it is difficult to distinguish lymphomas from other mediastinal masses. The presence of pleural effusion on radiography suggests lymphoma.2 A computed tomography (CT) scan and lymph node biopsy can also help with the diagnosis.
A pneumothorax may lead to the sudden onset of dyspnea and pleuritic chest pain. Radiography shows a radiolucent line of the pleura. Spontaneous pneumothorax is more common in men, and smoking is a primary risk factor.
Thymomas are the most common tumors found in the anterior mediastinum, accounting for up to 50 percent of these tumors.2,9,10 Patients with thymomas may have cough, chest pain, and dyspnea. Weight loss, anorexia, and fatigue may also occur. Approximately 50 percent of patients with thymomas have myasthenia gravis; however, only 10 to 15 percent of patients with myasthenia gravis have thymomas. Chest radiography shows a solid mass, and a CT scan shows a well-defined, encapsulated mass.2,9
A small percentage of anterior mediastinal masses are from thyroid enlargement (mediastinal goiter). Like those of other mediastinal masses, symptoms of thyroid goiter are caused by compromise of surrounding structures. Common symptoms include dysphagia, choking, and throat fullness.2 Radiography may show a mass effect. Thyroid goiters are encapsulated, lobulated tumors that are clearly visible on CT scan. Thyroid tests, such as thyroid ultrasonography or nuclear scan of the thyroid, can help confirm the diagnosis.10
Summary Table
| Condition | Radiography findings |
|---|---|
| Lymphoma | Pleural effusion |
| Pneumothorax | Radiolucent line of the pleura |
| Teratoma | Slow growing; large, round, lobulated mass with sharp margins; calcifications are most characteristic; often found incidentally |
| Thymoma | Well-defined, solid mass; often found incidentally |
| Thyroid goiter | Mass effect |
