Family physicians commonly diagnose and manage penile cutaneous lesions. Noninfectious lesions may be classified as inflammatory and papulosquamous (e.g., psoriasis, lichen sclerosus, angiokeratomas, lichen nitidus, lichen planus), or as neoplastic (e.g., carcinoma in situ, invasive squamous cell carcinoma). The clinical presentation and appearance of the lesions guide the diagnosis. Psoriasis presents as red or salmon-colored plaques with overlying scales, often with systemic lesions. Lichen sclerosus presents as a phimotic, hypopigmented prepuce or glans penis with a cellophane-like texture. Angiokeratomas are typically asymptomatic, well-circumscribed, red or blue papules, whereas lichen nitidus usually produces asymptomatic pinhead-sized, hypopigmented papules. The lesions of lichen planus are pruritic, violaceous, polygonal papules that are typically systemic. Carcinoma in situ should be suspected if the patient has velvety red or keratotic plaques of the glans penis or prepuce, whereas invasive squamous cell carcinoma presents as a painless lump, ulcer, or fungating irregular mass. Some benign lesions, such as psoriasis and lichen planus, can mimic carcinoma in situ or squamous cell carcinoma. Biopsy is indicated if the diagnosis is in doubt or neoplasm cannot be excluded. The management of benign penile lesions usually involves observation or topical corticosteroids; however, neoplastic lesions generally require surgery.
The diagnosis and management of penile cutaneous lesions can be challenging for some physicians because of a lack of familiarity and patient embarrassment. Despite these challenges, primary care physicians are capable of diagnosing and managing many penile lesions, and determining which patients require subspecialist referral. Noninfectious lesions may be classified as inflammatory and papulosquamous, or neoplastic.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References | Comments |
|---|---|---|---|
| Daily application of topical ultrapotent corticosteroid therapy for penile lesions should be limited to two weeks, followed by weekend dosing. Long-term follow-up should monitor for atrophy. | C | 9–11 | Observational studies and consensus guidelines |
| Lichen sclerosus (balanitis xerotica obliterans) requires long-term follow-up to monitor for malignant transformation. | C | 18 | Observational studies and expert opinion |
| Biopsy is appropriate for a penile lesion if the diagnosis is unclear, or if carcinoma in situ or squamous cell carcinoma are possible. | C | 18, 20 | Case series and expert opinion |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.xml.
Because many penile cutaneous lesions are diagnosed on physical examination, primary care physicians should be proficient in the genitourinary examination.1 The key to narrowing a differential diagnosis is defining the predominant characteristic of the lesions (Table 1). Most papules are benign, whereas ulcers or irregularly shaped masses may suggest malignancy. However, there are exceptions to both rules. Lesions localized to the penis usually involve different diagnostic and treatment considerations than lesions with extended or systemic findings. Biopsy is usually reserved for an unclear diagnosis, or if neoplasm is a consideration. Management options for noninfectious lesions are summarized in Table 2.
Table 1. Differential Diagnosis of Penile Lesions
| Lesion | Characteristic symptoms | Typical clinical appearance | Differential diagnosis |
|---|---|---|---|
| Inflammatory and papulosquamous lesions | |||
| Angiokeratomas | Asymptomatic | Red or blue papules; may appear only on the glans penis or also on the scrotum, groin, thighs, and abdominal wall | Pearly papules |
| Lichen nitidus | Asymptomatic | Pinhead-sized, hypopigmented papules; often extragenital | Herpes simplex virus, pearly papules |
| Lichen planus | Pruritus, soreness | Flat-topped, polygonal, violaceous papules; often extragenital | Secondary syphilis |
| Lichen sclerosus | Phimosis, painful erections, obstructive voiding, itching, pain, bleeding | Hypopigmented, thinned, phimotic prepuce; texture similar to cellophane; isolated to prepuce and glans penis | Carcinoma in situ, leukoplakia, scleroderma |
| Psoriasis | Pruritus | Red or salmon-colored, papulosquamous, circinate plaques that are often associated with white or silvery scales; usually systemic | Carcinoma in situ |
| Infectious lesions | |||
| Genital herpes | Primary disease: constitutional symptoms followed by genital vesicles Recurrent disease: prodromal local paresthesias, pruritus, burning sensation, hypersensitivity | Vesicles on an erythematous base that become a pustule before crusting over; heals without scarring; isolated to dermatome | Lichen nitidus |
| Human papillomavirus lesions | Asymptomatic | Exophytic, flesh-colored, warts; lobulated or irregular surface; may appear on perineum and perianal area; diagnosis confirmed by culture, DNA detection with polymerase chain reaction, or biopsy | Squamous cell carcinoma |
| Primary syphilis lesions | Painless | Ulcer (chancre); isolated; darkfield microscopy is needed for diagnosis | Zoon balanitis |
| Scabies | Pruritus that is worse at night; family members or other close contacts are affected | Genital burrows; may become superinfected and crusted; may appear on fingers Detection of mite, egg, or pellet confirms diagnosis | Psoriasis |
| Neoplastic lesions | |||
| Carcinoma in situ (erythroplasia of Queyrat, Bowen disease) | Pruritus, pain | Variable appearance; plaque or ulcer isolated to glans penis, prepuce, and other areas of the penis; biopsy needed for diagnosis | Psoriasis, lichen sclerosus, Zoon balanitis, invasive penile cancer, lichen planus, herpes simplex virus, syphilis, group B streptococcal balanitis, candidiasis, Reiter syndrome |
| Invasive squamous cell carcinoma | Delayed presentation, usually painless | Exophytic or endophytic appearance; presentation varies; local or metastatic; biopsy is needed for diagnosis | Giant condyloma (human papillomavirus) |
Table 2. Management Options for Noninfectious Penile Lesions
| Diagnosis | Primary management option | Alternate option |
|---|---|---|
| Inflammatory and papulosquamous lesions | ||
| Angiokeratoma | Observation | Surgery, cryoablation, electrocautery, laser ablation |
| Lichen nitidus | Observation | Topical corticosteroids, vitamin A analogues, cyclosporine (Sandimmune), itraconazole (Sporanox), phototherapy |
| Lichen planus | Topical corticosteroids | Circumcision for isolated prepuce lichen planus |
| Lichen sclerosus | Topical corticosteroids | Circumcision for isolated prepuce lichen sclerosus |
| Psoriasis | Topical corticosteroids | Vitamin D3 analogues, tacrolimus (Protopic), or pimecrolimus (Elidel) |
| Neoplastic lesions | ||
| Carcinoma in situ | Circumcision for isolated prepuce lesions | Mohs micrographic surgery Topical imiquimod (Aldara) |
| Invasive squamous | Circumcision for isolated prepuce lesions Mohs micrographic surgery for nonisolated lesions | Partial or radical penectomy Laser therapy, radiation, and brachytherapy have been attempted as alternatives |
Inflammatory and Papulosquamous Lesions
PSORIASIS
Psoriasis may occur at any age, with bimodal peaks at 16 to 22 years of age and at 57 to 60 years of age.2,3 The prevalence of psoriasis in the United States is 1 to 2 percent,4 with genital involvement occurring in up to 40 percent of patients.3,5–7 Psoriasis presents as red or salmon-colored, papulosquamous, circinate plaques (Figure 1), often associated with white or silvery scales.2,5 Pruritus and psychosocial distress are common. Exacerbating factors include stress, excessive alcohol and tobacco use, acute infections (particularly streptococcal), and some medication use (e.g., beta blockers, lithium).8 Extragenital psoriasis occurs on the extensor surfaces of elbows and knees, scalp, lumbosacral region, umbilicus, and nails. Psoriatic arthritis occurs in up to 25 percent of patients.
Figure 1.

Psoriasis. Salmon-colored papulosquamous plaque with silvery scales.
Psoriasis is usually clinically apparent in the presence of nail pitting or confirmatory lesions elsewhere on the body.3 Punch or shave biopsy is indicated if lesions are atypical. Treatment depends on whether the disease is localized or disseminated.3,5,7,9 First-line localized treatment includes mild to midstrength topical corticosteroids.3,6,8,9 Once-daily application of corticosteroids is sufficient because genital skin is permeable, and corticosteroid receptors remain saturated for almost 24 hours. As a general rule, no more than 50 g of ultrapotent or 100 mg of potent topical corticosteroids should be applied over a long-term period9 because continuous use may cause skin atrophy. Lesions may reappear when corticosteroid use is discontinued.10 To avoid overdose, daily ultrapotent topical corticosteroid use should be limited to two weeks, followed by weekend dosing.10 If long-term therapy is required, tacrolimus (Protopic) or pimecrolimus (Elidel) may be appropriate, without the risk of atrophy.11 Vitamin D3 analogues are a first-line option for localized disease, and are usually applied once or twice daily. Patients with refractory disease should be referred to a dermatologist.
LICHEN SCLEROSUS
Penile lichen sclerosus, also known as balanitis xerotica obliterans, occurs in males of all ages.12 The average age at diagnosis is 42 years.13–15 The estimated prevalence may be as high as one in 300 males.16,17 Lichen sclerosus is associated with squamous cell carcinoma in 4 to 6 percent of patients.6,14,18 Many physicians consider genital lichen sclerosus in males to be a precancerous condition that is similar to its counterpart in females.12,16
Lichen sclerosus appears as a hypopigmented lesion with a skin texture similar to crinkled paper or cellophane. It primarily affects the glans penis and prepuce (Figure 2). Bullae, erosions, or atrophy may be prominent. Patients typically present with phimosis, painful erections, obstructive voiding, itching, pain, and bleeding.16,19 Because the progression of the lesions may lead to obstruction, urinary retention may be the initial complaint.16,18,20 Almost all parts of the body can be affected, although they may be asymptomatic.12,16,20 Lichen sclerosus should be differentiated from carcinoma in situ (Figure 3), leukoplakia, and scleroderma.16,20
Figure 2.

Lichen sclerosus (balanitis xerotica obliterans). Hypopigmented lesion, atrophy, and phimosis.
Figure 3.
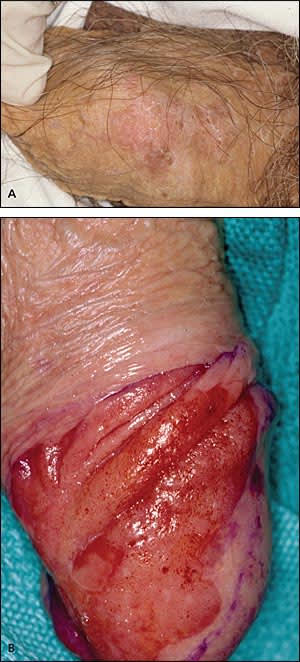
Carcinoma in situ. (A) Bowen disease presenting as erythematous plaque with soft, white scales; appearance is similar to psoriasis. (B) Characteristic raised, beefy red, velvety plaque.
The goal of treatment is to reduce symptoms and prevent malignant transformation.13 Lichen sclerosus can be treated with moderate to ultrapotent fluorinated topical corticosteroids. Biopsy is indicated if squamous cell carcinoma is suspected.20 Surgery is needed in patients with persistent disease or a history of squamous cell carcinoma.18 Circumcision may be indicated in patients with lichen sclerosus limited to the glans penis and prepuce. Severe cases may require reconstructive surgery,16,19 although conservative management may be appropriate if the risks of surgery outweigh the potential benefits.16 Systemic agents, such as retinoids, are reserved for severe cases of lichen sclerosus and when local therapy fails.19 Long-term follow-up is appropriate to monitor for malignant transformation.18
ANGIOKERATOMAS
The prevalence of angiokeratomas is unknown, but is believed to be less than 1 percent.21 These lesions occur more often in men than women, and are more common in white persons. Angiokeratomas are benign, well-circumscribed, red or blue papules measuring 1 to 6 mm that typically occur in patients older than 40 years.22–25 The diagnosis is usually made by characteristic appearance, although it may be misdiagnosed as penile cancer or pearly papules. Angiokeratomas may affect only the glans penis, or they may also affect the scrotum, groin, thighs, and abdominal wall26 (Figure 4). Patients with angiokeratomas may experience rare intermittent bleeding, pain, or pruritus.27 Angiokeratomas affecting the penile shaft, suprapubic region, and sacrum are associated with Fabry disease and should prompt referral.28 Treatment is indicated if the patient is symptomatic or if the lesions bleed. Options include surgery, cryoablation, electrocautery, and laser ablation.22,29,30 Treatment may be difficult in patients with extensive lesions.
Figure 4.

Angiokeratomas. Multiple blue papules; lesions may be red with a verrucous appearance.
LICHEN NITIDUS
Lichen nitidus is uncommon. The diagnosis is made on examination. Patients with lichen nitidus present with discrete, slightly elevated, hypopigmented papules measuring approximately 1 mm31,32 (Figure 5). These lesions should be distinguished from pearly papules, which have a ring-like distribution on the coronal sulcus (Figure 6). Lichen nitidus papules may occur on the penis, as well as the upper limbs and abdomen.31,33 Patients are typically asymptomatic and do not require treatment.31,33 Patients rarely experience pruritus.32,33 The course of lichen nitidus is variable and can resolve spontaneously.31 When treatment is indicated for cosmesis, options include corticosteroids, vitamin A analogues, cyclosporine (Sandimmune), itraconazole (Sporanox), and phototherapy.33 Laser ablation should be avoided because of the potential for scarring.31
Figure 5.

Lichen nitidus. Multiple pinhead-sized, slightly elevated, discrete, hypopigmented papules.
Figure 6.

Pearly papules. Distribution of multiple, small, dome-shaped, skin-colored papules with ring-like distribution on the coronal sulcus.
LICHEN PLANUS
Lichen planus is also uncommon. It is typically systemic, affecting mucous membranes, nails, acral sites, and the scalp.34 One fourth of patients with lichen planus have lesions on the genitalia, and most patients also have extra-genital involvement.35 Lichen planus lesions are raised, violaceous, flat-topped, polygonal papules36 (Figure 7). Fine white streaks (Wickham striae) may appear on the surface of the lesions. In uncircumcised patients, the lesions assume a lacy, white, reticulated pattern. Patients with lichen planus often complain of pruritus and soreness. Lesions may be associated with ulceration.34 Ulcerated or indurated lesions may suggest squamous cell carcinoma and require a biopsy.37
Figure 7.

Lichen planus. Raised, violaceous, flat-topped, polygonal papules.
The response to treatment of lichen planus is variable.37,38 Daily potent topical corticosteroids are usually effective but carry a risk of atrophy; however, weekend dosing of ultrapotent topical corticosteroids may be effective. For isolated lichen planus of the prepuce, circumcision is indicated when medical management fails.39
Neoplastic Lesions
CARCINOMA IN SITU
Penile carcinoma in situ is a premalignant lesion restricted to the skin. It typically affects uncircumcised men older than 60 years. Velvety plaques of the glans penis are known as erythroplasia of Queyrat. Keratotic plaques are known as Bowen disease (Figure 3A), which occurs on the penile shaft, scrotal skin, or perineum.6,19 Human papilloma virus (HPV) is the primary etiology of penile carcinoma in situ, although other factors may include smegma and trauma from friction, heat, and inflammation.40 Penile carcinoma in situ progresses to squamous cell carcinoma in approximately 5 to 30 percent of patients.41,42
Pruritus and pain occur in approximately 50 percent of patients with penile carcinoma in situ.41 Lesions usually appear as raised, beefy red, velvety, irregularly shaped plaques that may ulcerate (Figure 3B). The lesions are generally 2 to 35 mm in size and occur on the glans penis, urethral meatus, frenulum, coronal sulcus, and prepuce. In uncircumcised men, the lesions may be encrusted without a velvety appearance. Lesions on the shaft may appear erythematous; display fissuring; and have soft, white scales. Biopsy is needed for the diagnosis of penile carcinoma in situ; shave biopsy is generally adequate.
Lesions restricted to the prepuce are treated with circumcision. Mohs micrographic surgery is indicated for other penile carcinoma in situ lesions.40 Treatment with fluorouracil, curettage, local excision, or laser ablation is associated with significant recurrence rates. Radiation may be an option for patients who are not surgical candidates or who refuse surgery. Imiquimod (Aldara) is an immune response modifier that has also been studied as a treatment option for penile carcinoma in situ.40
Penile carcinoma in situ can be difficult to distinguish from other lesions, such as psoriasis. The differential diagnosis includes Zoon balanitis, a condition of unknown etiology usually affecting men 50 to 62 years of age.6,43,44 Zoon balanitis lesions generally appear as bright red or brown, shiny patches with red specks or as pinpoint red spots.6,40,44 Characteristic patches are sharply demarcated, glistening red, and occur on the glans penis, inner prepuce, or coronal sulcus44,45 (Figure 8). Lesions tend to bleed and may erode. Although Zoon balanitis is benign, the lesions may mimic carcinoma in situ; therefore, biopsy is needed.6,19,36
Figure 8.

Zoon balanitis. Characteristic well-demarcated red patch.
INVASIVE SQUAMOUS CELL CARCINOMA
Penile cancer is rare, with a prevalence of two or three cases per 100,000 men. The peak incidence is in men older than 70 years.42 Squamous cell carcinoma accounts for 95 percent of penile cancers.40,42 Risk factors include some types of HPV infection, lichen sclerosus, smegma, smoking, older age, poor hygiene, presence of foreskin, and phimosis.6,19,40 Giant condyloma (Figure 9) may be difficult to distinguish from squamous cell carcinoma, and biopsy is indicated if the diagnosis is in doubt.
Figure 9.

Giant condyloma. Appearance is similar to exophytic squamous cell carcinoma.
The presentation of squamous cell carcinoma is variable because patients commonly delay seeking medical care, with average delays of six months or longer.42,46,47 In the early stages, squamous cell carcinoma can present as a painless lump or ulcer that progresses to thickened skin and a wart-like growth, sometimes associated with foul discharge (Figure 10A). Rashes and changes in skin coloration may occur.48 Exophytic or fungating squamous cell carcinoma typically appears as a large, irregularly shaped mass, whereas endophytic squamous cell carcinoma commonly presents as ulcerative and infiltrating lesions.42,49 Exophytic lesions occasionally lead to phimosis with the mass not visible until the prepuce is retracted (Figure 10B).
Figure 10.
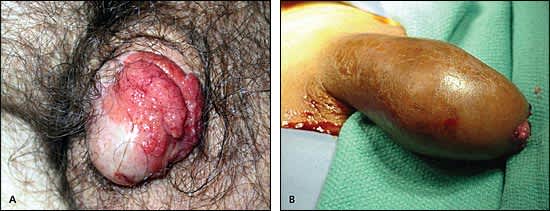
Squamous cell carcinoma. (A) A painless lump with wart-like growth is common. (B) A large mass under the prepuce may cause phimosis; the lesion is not visible unless the prepuce is retracted.
The diagnosis of squamous cell carcinoma is confirmed with biopsy. The lesion size determines whether incisional or excisional biopsy should be performed.42 Treatment options have not been compared in randomized trials because of the rarity of the disease. In general, low-grade and low-stage tumors can be treated with organ-sparing techniques, such as Mohs micrographic surgery. Lesions restricted to the prepuce are generally best treated by circumcision.42 Partial penectomy, laser therapy, radiation, and brachytherapy have been attempted as alternatives to radical penectomy.6,40,49 However, penile amputation is the standard treatment for higher-stage tumors (i.e., T2 to T4).42,49 Patients should receive lifelong surveillance for recurrence.
