A 23-year-old man presented with right hip pain that had worsened over four weeks. He was a member of his college's soccer team, but had no history of falls or recent trauma. He had similar hip pain two years earlier that was self-limited, but the rest of his medical history was unremarkable. He had no bowel or bladder symptoms. Although over-the-counter pain medication was initially effective, he was eventually unable to play soccer.
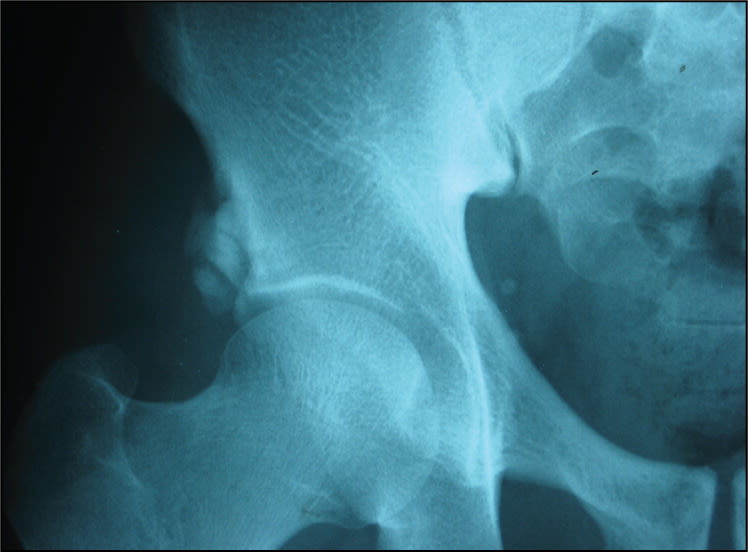
On physical examination, the patient walked with an antalgic gait. He was afebrile and had normal vital signs. His musculoskeletal examination revealed normal spinal curvature, nontender pelvic region, and equal leg length. He had tenderness with extreme flexion and rotation of the right hip, which reduced his range of flexion. Range of motion in the other joints was normal. Pelvic radiography was performed (Figures 1 and 2).
Figure 1.

Figure 2.
Question
Based on the patient's history, physical examination, and radiography findings, which one of the following is the most likely diagnosis?
A. Avulsion fracture of anterior inferior iliac spine.
B. Calcific tendinitis of the rectus femoris.
C. Myositis ossificans of the rectus femoris.
D. Synovial sarcoma.
Discussion
The answer is B: calcific tendinitis of the rectus femoris. The rectus femoris is the only one of the quadriceps muscles to cross the hip joint, which allows it to act as a hip flexor and a knee extensor. The rectus femoris has two heads: the anterior head, which originates from the anterior inferior iliac spine, and the reflected or posterior head, which originates from a groove above the acetabular ring. The rectus femoris attaches to the base of the patella.
The patient's radiographs show opacifications (calcific deposits) in a clustered pattern at the anterior inferior iliac spine, just above the right acetabular rim. The comet-tail appearances of these opacifications suggest that the calcific deposits lie within the tendons. Computed tomography (CT) or magnetic resonance imaging (MRI) can confirm the diagnosis.
Groin injuries account for 2 to 5 percent of all sports injuries and 5 to 7 percent of injuries in soccer players.1 Diagnosis starts with a patient history detailing repetitive strain and pain with hip flexing activities. Physical examination reveals tenderness with full flexion of the hip and adduction, thus stretching, of the rectus femoris muscle.
Treatment of rectus femoris tendinitis includes rest, antiinflammatory medications, and physical therapy until the pain resolves. Therapeutic ultrasound, and CT-guided analgesic and steroid injections have all been used with similar results.2 Patients with avulsion fracture of the anterior inferior iliac spine present with acute pain in the anterior lateral aspect of the groin with limited hip flexion after injury. Radiography shows a clear disruption in the bony cortex. The condition is treated with rest, and the patient may return to exercise as pain permits.3
Myositis ossificans of the quadriceps muscle is common in contact sports. The muscle is crushed against the bone, and improper treatment leads to bone formation within the muscle. Radiography shows bone formation approximately two to four weeks after the injury. Myositis ossificans is usually treated with rest, but may require excision.4
Synovial sarcoma is a soft tissue tumor. Examination usually reveals a palpable, mildly tender mass with or without a history of trauma. Plain radiography findings are often normal, but MRI shows an ill-defined lesion at the musculotendinous junction of the rectus femoris muscle. Biopsy and excision are needed for diagnosis and management.5
Summary Table
| Condition | Characteristics |
|---|---|
| Avulsion fracture of anterior inferior iliac spine | Acute pain in the anterior lateral aspect of the groin, limited hip flexion, radiography shows clear disruption in the bony cortex |
| Calcific tendinitis of rectus femoris | Repetitive strain injury, radiography shows calcium deposits at the musculotendinous junction |
| Myositis ossificans of the rectus femoris | Bone formation within the rectus muscle following crush injury to the quadriceps muscle, radiography shows opacifications within the muscle mass |
| Synovial sarcoma | Soft tissue tumor, magnetic resonance imaging shows ill-defined lesion, normal plain radiography findings |
