A 61-year-old woman presented with a history of chronic pain and stiffness in multiple joints. She had morning stiffness in her hands, hips, and knees that gradually improved with activity. She did not report any foot pain or stiffness, fever, or rash.
On examination she had swelling around the distal interphalangeal joints in multiple fingers with relative sparing of the proximal and metacarpophalangeal joints (Figure 1). The joints were not warm or tender to palpation. Laboratory studies showed normal values of rheumatoid factor and anticyclic citrullinated peptide, and a normal white blood cell count. Hand radiography was ordered (Figure 2).
Figure 1.
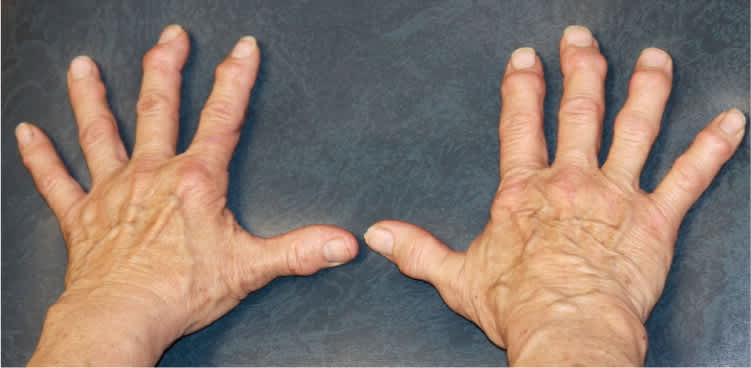
Figure 2.

Question
Based on the patient's history, physical examination, and radiographic findings, which one of the following is the most likely diagnosis?
A. Gouty arthritis.
B. Osteoarthritis.
C. Psoriatic arthritis.
D. Rheumatoid arthritis.
Discussion
The correct answer is B: osteoarthritis. Heberden nodes (hard or bony swellings in the distal interphalangeal joints) along with a deviated distal finger are a classic finding in osteoarthritis. The patient has a variant form of the condition known as erosive osteoarthritis that is common in postmenopausal women. The radiograph of her hands shows subchondral sclerosis and the “gull wing” deformity in the distal interphalangeal joint of the left middle finger (Figure 3). The gull wing deformity is indicative of this variant form.1 Swelling and erosive changes of the proximal interphalangeal joints (Bouchard nodes) often occur in patients with osteoarthritis, but were not present in this patient.
Figure 3.

Radiograph of patient with erosive osteoarthritis showing “gull wing” deformity in the distal interphalangeal joint of the left middle finger (arrow).
Osteoarthritis is the most common cause of progressive, arthritic disease.2 It affects millions of Americans and is the most common cause of disability in the United States. The erosive form of osteoarthritis is more common in women, with an estimated female-to-male ratio of 12:1, whereas the generalized form has a female-to-male ratio of 10:1.3,4
Patients with osteoarthritis have a decrease in chondrocyte response to growth factors that stimulate joint repair after repetitive joint stress.5 The acute phase is characterized by inflamed, tender joints and osteophyte formation around the joint margins.6 As the patient progresses into the chronic phase, inflammatory changes subside and the joints become painless to palpation. Bony outgrowths continue to form, resulting in the development of Heberden nodes.
Gouty arthritis is an intermittent, inflammatory arthritis that usually presents acutely as a red, swollen, warm, and painful joint. The metatarsophalangeal joint is most commonly affected (podagra).7 Monosodium urate monohydrate crystal deposition leads to stiffness, swelling, and periarticular subcutaneous nodules (tophi). Radiographic findings include erosive, sclerotic margins with lytic “rat bite” lesions. Laboratory work may show elevated uric acid levels during an acute attack, but the diagnosis is made by identifying crystals in joint fluid with negative birefringence under polarized light.
Psoriatic arthritis presents as painful, red, swollen joints in the fingers, but in conjunction with psoriasis of the skin or scalp.4 The joint swelling is secondary to inflammation of the ligaments and tendons, not skeletal changes. Men and women are equally affected, and patients may be positive for human leukocyte antigen-B27. Radiography shows joint erosion, spurs, and pencil-in-cup deformity.
Rheumatoid arthritis is an erosive, inflammatory arthritis that affects women three times more often than men.8 Patients present with symmetric stiffness in multiple joints, most often occurring in the morning, that lasts at least 45 minutes before subsiding.9 Joints are boggy, warm, and tender to palpation as in osteoarthritis, but lack erythema and rarely involve the distal interphalangeal joint. Elevated titers of rheumatoid factor and anticyclic citrullinated peptide antibodies, as well as erosive margins and joint-space narrowing on radiography, also help to differentiate rheumatoid arthritis from osteoarthritis. A “swan neck” deformity is present in chronic cases.
Summary Table
| Condition | Characteristics |
|---|---|
| Gouty arthritis | Monoarticular involvement, most commonly the metatarsophalangeal joint (podagra) with subcutaneous, periarticular nodules (tophi); red, swollen, warm, painful joint in acute attack; erosive, sclerotic margins with lytic “rat bite” lesions on radiography |
| Osteoarthritis | Polyarticular involvement with joint stiffness and swelling at the proximal interphalangeal joints (Bouchard nodes) and distal interphalangeal joints (Heberden nodes); radial deviation in the chronic phase; osteophyte formation with “gull wing” deformity on radiography |
| Psoriatic arthritis | Associated with psoriasis; inflammation of the tendons and ligaments leads to painful, red, swollen joints; joint erosion, spurs, and pencil-in-cup deformity on radiography |
| Rheumatoid arthritis | Symmetric stiffness in multiple joints in the morning that lasts at least 45 minutes; boggy, warm, tender joints, primarily involving the proximal interphalangeal and metacarpophalangeal joints; “swan neck” deformity in chronic cases; erosive margins and joint-space narrowing on radiography |
