Anaphylaxis is a severe, life-threatening, systemic allergic reaction that is almost always unanticipated and may lead to death by airway obstruction or vascular collapse. Anaphylaxis occurs as the result of an allergen response, usually immunoglobulin E–mediated, which leads to mast cell and basophil activation and a combination of dermatologic, respiratory, cardiovascular, gastrointestinal, and neurologic symptoms. Dermatologic and respiratory symptoms are most common, occurring in 90 and 70 percent of episodes, respectively. The three most common triggers are food, insect stings, and medications. The diagnosis of anaphylaxis is typically made when symptoms occur within one hour of exposure to a specific antigen. Confirmatory testing using serum histamine and tryptase levels is difficult, because blood samples must be drawn with strict time considerations. Allergen skin testing and in vitro assay for serum immunoglobulin E of specific allergens do not reliably predict who will develop anaphylaxis. Administration of intramuscular epinephrine at the onset of anaphylaxis, before respiratory failure or cardiovascular compromise, is essential. Histamine H1 receptor antagonists and corticosteroids may be useful adjuncts. All patients at risk of recurrent anaphylaxis should be educated about the appropriate use of prescription epinephrine autoinjectors.
Anaphylaxis is a life-threatening, systemic hypersensitivity reaction.1 It is the most severe form of allergic reaction and is almost always unexpected.2 Delay in clinical diagnosis and treatment may result in death by airway obstruction or vascular collapse.1 The incidence of anaphylaxis in the United States is 49.8 cases per 100,000 person-years.2 Lifetime prevalence is 0.05 to 2 percent, with a mortality rate of 1 percent.2,3 Compared with that of the general population, the risk of anaphylaxis is doubled in patients with mild asthma and tripled in those with severe disease.4 The true prevalence and mortality rates may be higher because of the unexpected nature of the disease, the lack of reliable confirmatory testing, confusion over the clinical definition, and underreporting by physicians.4,5 Patients may arrive at a physician's office remote from an event or with active symptoms, or they may develop anaphylaxis after administration of common treatments used in the clinic. Family physicians and patients need to be prepared to recognize and quickly treat anaphylaxis to prevent potentially catastrophic outcomes.5,6
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| The clinical history is the most important tool to determine whether a patient has had an anaphylactic reaction and the cause of the episode. | C | 1, 3, 5, 6 |
| Intramuscular epinephrine (1:1,000 dilution dosed at 0.01 mg per kg [maximal dose of 0.3 mg in children and 0.5 mg in adults]), along with appropriate management of airway, breathing, and circulation, is the first and most important therapeutic option in the treatment of anaphylaxis. | B | 1, 3, 5–7, 9, 10, 12–19 |
| Volume replacement with normal saline is crucial in the treatment of hypotension that does not respond to epinephrine. | B | 1, 3, 5, 6, 9, 12–15 |
| Histamine H1 receptor antagonists and corticosteroids may be helpful as second-line treatments in patients with anaphylaxis. | C | 1, 3, 5, 6, 19, 24, 25 |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.xml.
Triggers and Pathophysiology
Anaphylaxis is a systemic response to a specific allergen, usually occurring within one hour of exposure. The most common triggers are food, insect stings, and medications (Table 1).5,6 Food-related reactions are most common in children up to four years of age, and medication reactions are most common in patients older than 55 years.2
Table 1. Possible Triggers of Anaphylaxis
| Allergy testing and allergy-specific immunotherapy | |
| Animal dander | |
| Foods | |
| Egg, fish, food additives, milk, peanuts, sesame, shellfish, tree nuts | |
| Idiopathic anaphylaxis (always a diagnosis of exclusion; consider unrecognized allergen or mastocytosis) | |
| Insect venom | |
| Stinging insects from the Hymenoptera order (e.g., bee, wasp, fire ants) | |
| Latex and other occupational allergens | |
| Medications | |
| Allopurinol (Zyloprim), angiotensin-converting enzyme inhibitors, antibiotics (beta-lactams most common), aspirin, biologic modifiers (e.g., interferon), nonsteroidal anti-inflammatory drugs, opioids | |
| Physical factors (very rare) | |
| Cold, heat, exercise, sunlight | |
| Radiocontrast media | |
Most cases of anaphylaxis are immunoglobulin E (IgE)–mediated. Antibodies exposed to a particular allergen attach to mast cells and basophils, resulting in their activation and degranulation. A variety of chemical mediators are released including histamine, heparin, tryptase, kallikrein, platelet-activating factor, bradykinin, tumor necrosis factor, nitrous oxide, and several types of interleukins.5,6
Historically, anaphylaxis-type reactions triggered by the direct activation of the mast cell (e.g., radiocontrast media reactions) were referred to as anaphylactoid reactions. Currently, immune and nonimmune anaphylaxis are the preferred terms to differentiate between IgE-mediated reactions and direct activation reactions.1,5 This distinction matters little in the acute clinical setting, because the treatment is the same for both types of reactions. However, the difference is important when deciding on prevention strategies, such as immunomodulation therapy.5,6
Diagnosis
CLINICAL PRESENTATION
Table 2 lists possible manifestations of anaphylaxis for each body system.5,7 Signs and symptoms usually develop within five to 30 minutes of exposure to the offending allergen, but may not develop for several hours.3,5,6 A biphasic reaction is a second acute anaphylactic reaction occurring hours after the first response and without further exposure to the allergen.5,8 One to 20 percent of patients with anaphylaxis experience biphasic reactions, which usually occur within eight hours of the initial reaction, but may occur as late as 24 to 72 hours after exposure.8,9
Table 2. Manifestations of Anaphylaxis by Body System
| Dermatologic/mucosal |
| Eyes: periorbital swelling/erythema, injected conjunctiva, tears |
| Oral mucosa: angioedema of the tongue and lips |
| Skin: urticarial rash, pruritus or flushing, morbilliform rash, piloerection, angioedema |
| Respiratory |
| Lower airway: bronchospasm with wheezing or cough, chest tightness, tachypnea, decreased peak expiratory flow, cyanosis, respiratory collapse/arrest |
| Upper airway: sensation of throat constriction; dry cough; difficulty breathing, swallowing, speaking; changes in voice; stridor; cyanosis; respiratory collapse/arrest |
| Cardiovascular |
| Early: tachycardia, diaphoresis, delayed capillary refill, hypotension |
| Late: bradycardia, shock, T-wave inversion and ST depression in multiple leads, cyanosis, cardiac arrest |
| Gastrointestinal |
| Nausea, vomiting, diarrhea, abdominal cramps |
| Neurologic |
| Throbbing headache, dizziness, lightheadedness, confusion, tunnel vision, loss of consciousness |
| General |
| Anxiety, feeling of impending doom, metallic taste, paresthesia in extremities, malaise, weakness |
| In children: sudden behavior changes, irritability, cessation of play |
note: Manifestations are listed in order of clinical importance/frequency.
In 2004, the Second Symposium on the Definition and Management of Anaphylaxis developed clinical criteria for diagnosing anaphylaxis in the acute setting (Table 3).10 The presence of one of three criteria predicts diagnosis of anaphylaxis 95 percent of the time.3,10 The clinical history is the most important tool to determine whether a patient has had an anaphylactic reaction and the cause of the episode.1,3,5,6
Table 3. Clinical Criteria for Diagnosing Anaphylaxis
| Anaphylaxis is highly likely when any one of the following three sets of criteria is fulfilled: | |
| 1. Acute onset of an illness (minutes to several hours) with involvement of the skin, mucosal tissue, or both (e.g., generalized hives; pruritus or flushing; swollen lips, tongue, or uvula), and at least one of the following: | |
| Respiratory compromise (e.g., dyspnea, wheeze-bronchospasm, stridor, reduced peak expiratory flow, hypoxemia) | |
| Reduced blood pressure or associated symptoms of end-organ dysfunction (e.g., hypotonia [collapse], syncope, incontinence) | |
| 2. Two or more of the following that occur rapidly (minutes to several hours) after exposure to a likely allergen for that patient: | |
| Involvement of the skin, mucosal tissue, or both (e.g., generalized hives; pruritus or flushing; swollen lips, tongue, or uvula) | |
| Respiratory compromise (e.g., dyspnea, wheeze-bronchospasm, stridor, reduced peak expiratory flow, hypoxemia) | |
| Reduced blood pressure or associated symptoms (e.g., hypotonia [collapse], syncope, incontinence) | |
| Persistent gastrointestinal symptoms (e.g., abdominal cramps, vomiting) | |
| 3. Reduced blood pressure that occurs rapidly (minutes to several hours) after exposure to a known allergen for that patient. | |
| Infants and children: low systolic blood pressure (age-specific)* or a more than 30 percent decrease in systolic blood pressure | |
| Adults: systolic blood pressure of less than 90 mm Hg or a more than 30 percent decrease from that person's baseline | |
*—Defined as less than 70 mm Hg in children one month to one year of age; less than 70 mm Hg + (2 × age) in children one to 10 years of age; and less than 90 mm Hg in those 11 to 17 years of age.
Adapted with permission from Sampson HA, Muñoz-Furlong A, Campbell RL, et al. Second Symposium on the Definition and Management of Anaphylaxis: summary report—second National Institute of Allergy and Infectious Disease/Food Allergy and Anaphylaxis Network Symposium. Ann Emerg Med. 2006;47(4):374.
Skin involvement, predominantly urticaria and angioedema, occurs in 90 percent of episodes.1,3,5,6 Respiratory manifestations are present in 70 percent of episodes, primarily with signs and symptoms of upper airway obstruction.1,3,5,6 Lower airway obstruction may occur, especially in patients with a history of asthma. Cardiovascular involvement, which could lead to life-threatening hypotension, occurs in 45 percent of patients.1,3,5,6 Gastrointestinal and neurologic involvement occur 45 and 15 percent of the time, respectively.1,3,5,6
DIFFERENTIAL DIAGNOSIS
Any condition that may result in the sudden, dramatic collapse of the patient, such as myocardial ischemia, pulmonary embolism, foreign body aspiration, acute poisoning, hypoglycemia, and seizure, can be confused with severe anaphylaxis. However, a vasovagal event is the most common condition confused with anaphylaxis.5,6 Bradycardia helps differentiate vasovagal events from anaphylaxis, because tachycardia is typical in the latter.3 However, tachycardia can transition into bradycardia during the end stages of a severe anaphylactic reaction when vascular collapse occurs.5,6
Additional diagnostic considerations include flushing syndromes in postmenopausal women, spicy food consumption, metastatic carcinoid tumors, and alcohol use in persons with aldehyde dehydrogenase deficiency.3,5,6 Mastocytosis, a rare condition involving overpropagation of mast cells to the point of organ infiltration, may present as anaphylaxis without a trigger.5 Psychiatric disorders, such as panic attack or severe generalized anxiety, can also be confused with anaphylaxis. Finally, patients may have urticaria, angioedema, and reactive airway symptoms occurring individually, without fulfilling the criteria for anaphylaxis.3,5,6,10
LABORATORY TESTING
Anaphylaxis is a clinical diagnosis.1,7 The value of confirmatory blood testing is limited.11 Two tests that have been evaluated for use in the acute setting are serum histamine and tryptase levels; elevations from baseline levels may be helpful in confirming anaphylaxis.7,11 Histamine levels must be obtained within one hour of symptom onset, and samples require special handling because histamine breaks down with any movement. Tryptase levels do not increase until 30 minutes after the onset of symptoms and peak at one to two hours; therefore, serial levels are sampled on presentation, one to two hours after presentation, and 24 hours after presentation to assess for a return to baseline.5–7,11
Allergen skin testing and in vitro assay for serum IgE of specific allergens do not reliably predict who will develop anaphylaxis.5,6 Allergen testing identifies sensitivity to an allergen, but not whether the patient will have a systemic reaction. Testing is more helpful after an episode of anaphylaxis to identify which allergen most likely caused the reaction and to promote future avoidance.1,3
Management of Acute Anaphylaxis
In the management of anaphylaxis, administering intramuscular epinephrine and ensuring proper oxygenation and effective circulation are key.3 A suggested office-based protocol is shown in Figure 1,9,12–15 and recommended equipment is listed in Table 4.9,12–15 Performing a primary survey and providing supportive care for the patient's airway, breathing, and circulation (with administration of epinephrine) are the critical initial steps. Patients should have easy access to commercially made, nonexpired epinephrine autoinjectors, which are preferred for delivering this therapy.9,12,16
Figure 1. Management of Anaphylaxis in the Outpatient Setting
Algorithm for the outpatient management of anaphylaxis.
Information from references 9, and 12 through 15.
Table 4. Equipment Recommended for Outpatient Management of Acute Anaphylaxis
| Commercially made epinephrine autoinjector (child and adult version) or aqueous epinephrine (1:1,000 dilution vials), autoinjector preferred |
| Injectable histamine H1 receptor antagonists |
| Injectable or oral corticosteroids |
| Intravenous start kit: tourniquets, large-bore catheters, alcohol swipes |
| Normal saline |
| Oxygen setup with different sized masks |
| Peak flow meter |
| Stethoscope and appropriately sized blood pressure cuff |
Securing the airway and providing 100 percent oxygen, when available, are crucial.9,12–15 Intravenous fluid administration is critical for all patients whose hypotension does not respond to epinephrine.1,3,5,6,9,12–15 Because of vascular dilation and increased permeability, with up to 35 percent of intravascular fluid shifting into the extravascular space,16 intravenous fluids should be administered through two large-bore catheters. In adults and adolescents, 2 L of normal saline are usually administered initially; more may be required in severe cases.9 Children should receive boluses of 10 to 20 mL per kg until hypotension is controlled.9,12–15 Even in the presence of upper airway obstruction, placing a patient in the recumbent position with the lower extremities raised is preferred over elevating the head of the patient's bed, because the vascular collapse during anaphylaxis can be devastating.9,15
The medications most commonly used for treatment of anaphylaxis are epinephrine, histamine H1 receptor antagonists, and corticosteroids.17,18 Current practice guidelines unanimously identify the timely administration of epinephrine, at initial diagnosis and ideally before respiratory failure or cardiovascular compromise, as the most important treatment for anaphylaxis.1,5–7,9,10,15–19 Epinephrine activates the α1 adrenergic receptors and β1 and β2 adrenergic receptors, leading to immediate vasoconstriction, increased peripheral resistance, decreased mucosal edema, increased cardiac inotropy/chronotropy, and bronchodilation, reversing the airway obstruction and vascular collapse.16 In a retrospective review of food-induced anaphylaxis in 13 children, all seven of the surviving patients received epinephrine within five minutes of severe respiratory symptoms, whereas the six who died did not.20
The window of therapeutic benefit of epinephrine is likely narrow, with several retrospective reviews demonstrating that delayed administration leads to poor outcomes.16–18 Common adverse effects of epinephrine at recommended doses include agitation, anxiety, tremulousness, headache, dizziness, pallor, and palpitations.16 Although concern may be warranted when giving epinephrine to older patients and patients with known coronary artery disease, there are no controlled studies that have weighed the risk,17 and at this time, best evidence shows that benefits far outweigh the risk.16,17
The preferred route of administration for epinephrine is intramuscular injection because it provides more reliable and quicker rise to effective plasma levels than the subcutaneous route.16–18 An intramuscular 1:1,000 aqueous solution of epinephrine at a dose of 0.01 mg per kg (maximal dose of 0.3 mg in children and 0.5 mg in adults) is given every five to 15 minutes until the patient is without symptoms of respiratory or vascular compromise.9,12–15 The onset of action is usually three to five minutes. The use of a commercially made autoinjector is preferred, because dosing errors are common when drawing epinephrine from a vial.21 Commercial devices allow for a set dose with the correct dilution (e.g., 0.15 mg for patients weighing less than 66 lb [30 kg]; 0.3 mg for patients weighing more than 66 lb).22,23 Intravenous epinephrine may be used to manage refractory anaphylaxis in consultation with an intensivist, because dosing requires close cardiovascular monitoring.17
Adjunct therapies include H1 receptor antagonists and systemic corticosteroids. H1 receptor antagonists are not effective first-line agents for anaphylaxis. Although they improve cutaneous erythema and decrease pruritus in the acute setting, they have not been shown to reverse upper airway obstruction or improve hypotension.24 With an onset of action of one to two hours, receptor antagonists, if given, should be used only as an adjunct to epinephrine and management of airway, breathing, and circulation. The limited benefits of H1 receptor antagonists need to be weighed against the risk of sedation in a potentially compromised patient.24 Because the onset of action is approximately six hours from administration, corticosteroids should not be used as a first-line treatment.15,20 Corticosteroids may be beneficial in preventing biphasic reactions.16,19,25
Patients with reactive airways disease and active bronchoconstriction require special consideration. If wheezing and coughing do not respond fully to epinephrine, these patients may benefit from receiving beta2 agonist nebulizers.1,5,6 Another population requiring special consideration includes patients on long-term beta-blocker therapy. These patients may have a blunted response to epinephrine and could benefit from glucagon (Glucagen; 3.5 to 5 mg intravenously once, repeat if no blood pressure response within 10 minutes).1,3,5,6
If a patient with anaphylaxis develops significant respiratory or circulatory symptoms (e.g., hypoxia, respiratory distress, hypotension), transport to a hospital must be arranged for continued therapy and monitoring. This is especially important when epinephrine administration is delayed and the patient's hypotension or airway obstruction does not resolve.1,5,6,10
In most cases of anaphylaxis, symptoms completely abate with intramuscular epinephrine. The physician will need to determine the length of postreaction monitoring. The unpredictable nature of biphasic reactions makes this decision difficult, and no guidelines address this issue.8 Reaction severity is not a predictor of biphasic reactions.9 The patient's ability to recognize symptoms and to self-administer epinephrine using an autoinjector should drive this decision. Ten hours of observation is probably adequate in most situations, but some investigators recommend a minimum of 24 hours.8,9
Postanaphylaxis Care
Following an anaphylactic reaction, appropriate education may be helpful for preventing and ameliorating future events. If a physician feels inadequately trained to provide such education, referral to an allergy specialist may be appropriate.9,16 Sometimes the patient presents remote from the event, and the offending allergen may be in question. In such cases, an allergy specialist may also be helpful in determining possible causes. Patients may choose to undergo allergy testing in a controlled environment to find the specific allergen to ensure avoidance and consideration for immunotherapy.1,3,5,6 Table 5 provides a list of preventive measures to reduce the risk of repeat episodes of anaphylaxis.9,12
Table 5. Preventive Measures to Reduce the Risk of Repeat Episodes of Anaphylaxis
| Patient measures | |
| Maintain a current and appropriately dosed epinephrine autoinjector near where the patient spends most of his or her time; take it when traveling and keep a placebo trainer for education | |
| Avoid the offending allergen | |
| Patients with food-induced anaphylaxis: use high scrutiny when reading ingredient lists and ask what is in the food prepared for them | |
| Patients with medication-induced anaphylaxis: avoid the offending medication and those with known cross activity; wear a medical alert bracelet to prevent administration of the offending medication | |
| Patients with insect-induced anaphylaxis: avoid known locations of the offending arthropods | |
| Physician measures | |
| Implement a waiting period of 20 to 30 minutes after the patient is given an injection of a medication or biologic agent; avoid administering injections if an alternative oral medication is available | |
| Optimize management of reactive airways and coronary artery disease | |
| Consider substituting other medications for those that may blunt the effect of epinephrine, such as beta blockers, angiotensin-converting enzyme inhibitors, angiotensin-II receptor blockers, tricyclic antidepressants, and monoamine oxidase inhibitors | |
Allergen avoidance is the mainstay of prevention, but may not be completely attainable, especially with insect and food allergies.1,3,10 A commercially made epinephrine autoinjector should be prescribed to all patients who have experienced anaphylactic reactions.9,12 When properly used, these devices can allow for early administration of epinephrine before refractory anaphylaxis develops.21 Patients should be instructed to call 911 or go to the nearest hospital for monitoring if they use their self-injectable device.9,12 The three commercially made devices in the United States are the Epipen, Twinject, and Adrenaclick. Physicians and patients should be familiar with their proper use. Several retrospective reviews have shown no permanent sequelae, and only rare need for any invasive treatment when injected inappropriately or in the wrong location.26–28
Figure 2 provides step-by-step instructions on how to use the current Epipen (released in 2008).29 A video can be viewed at http://www.youtube.com/watch?v=pgvnt8YA7r8&amo;playnext=1&amo;list=PLB36920D65D63755C.
Figure 2.
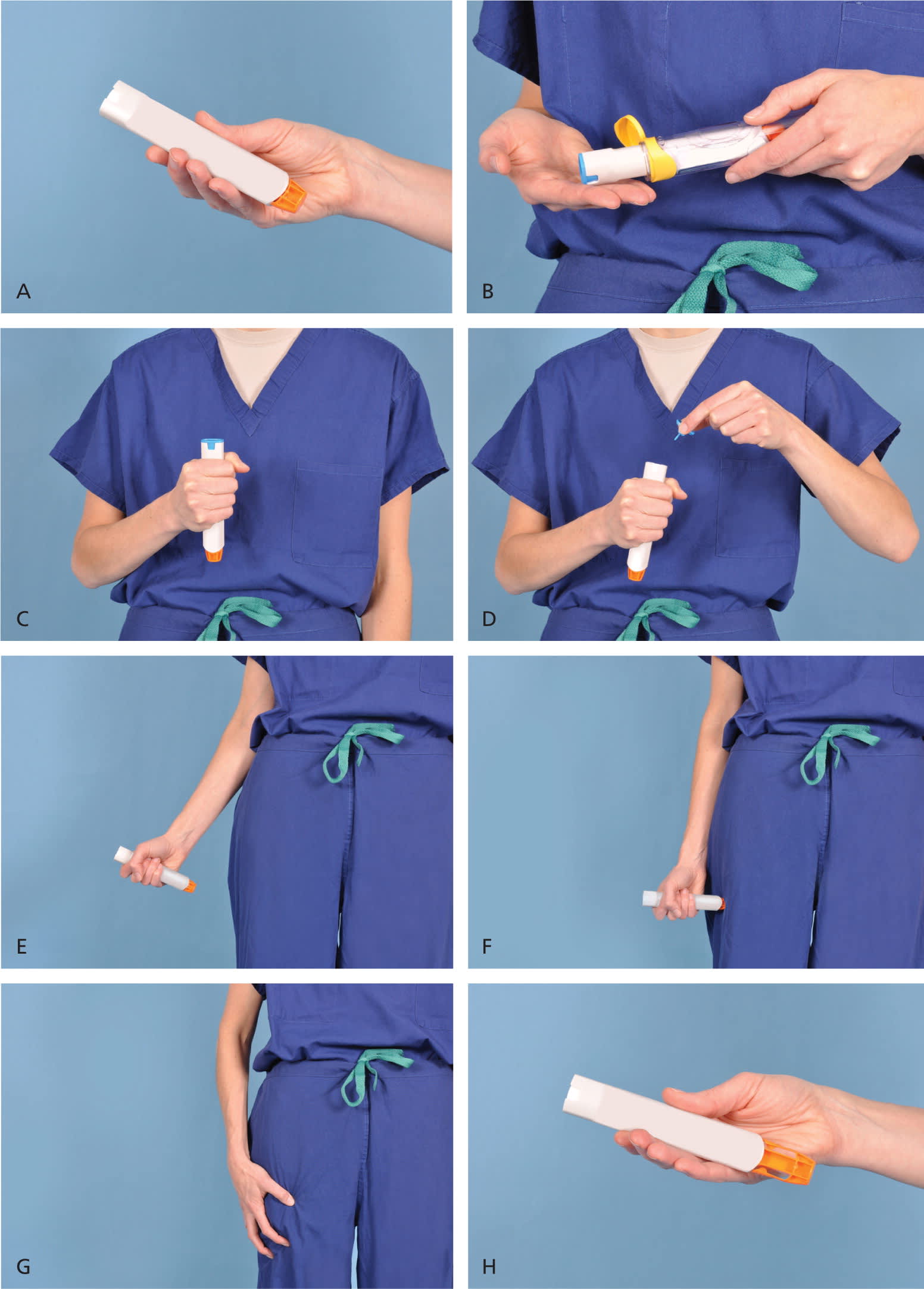
Demonstration of appropriate deployment of the (A) Epipen (released in 2008). For demonstration purposes, a trainer device is being used instead of a live device; however, the coloring of key components is the same as the actual adult device. (B) Open the yellow cap of the carrying case and remove the device from its storage tube (the Epipen Jr. has a green cap). (C) Grasp and form a fist around the unit with the orange tip facing down. (D) With the other hand, remove the blue safety release. (E) Aim the orange tip toward the outer thigh. (F) Swing the arm and jab the device firmly into the outer thigh, at a 90-degree angle, until the device clicks. The needle will deploy at this time into thigh (the autoinjector is designed to work through clothing). Hold the device firmly against the thigh for 10 seconds, so the entire dose will be delivered. (G) Remove the device from the thigh and massage the injection area for 10 seconds. (H) The safety feature of the device, extension of the orange tip that locks into place, will completely cover the needle immediately after use. The used device should be taken to the hospital emergency department with the patient for disposal.
Information from reference 29.
Data Sources: A PubMed search was completed in Clinical Inquires using the key terms anaphylaxis, epinephrine, epinephrine autoinjector, antihistamine, and steroids. The search included meta-analyses, systematic reviews, clinical guidelines, and clinical reviews. Also searched were the Agency for Healthcare Research and Quality evidence reports, Cochrane database, National Guideline Clearinghouse, Institute for Clinical Systems Improvement, MD Consult, and the U.S. Preventive Services Task Force. Search date: April 2, 2011.
