A 48-year-old serviceman deployed to Southwest Asia presented with a small, firm papule on the lateral edge of his left lower eyelid that he first noticed about three years earlier. The lesion had not significantly changed in size or color. He did not have pruritus, scaling, bleeding, or other skin symptoms. He also had no diplopia, visual deficits, fevers or chills, or other medical problems. His lifetime sun exposure was moderate, but he did not have a history of skin cancer or skin biopsies.
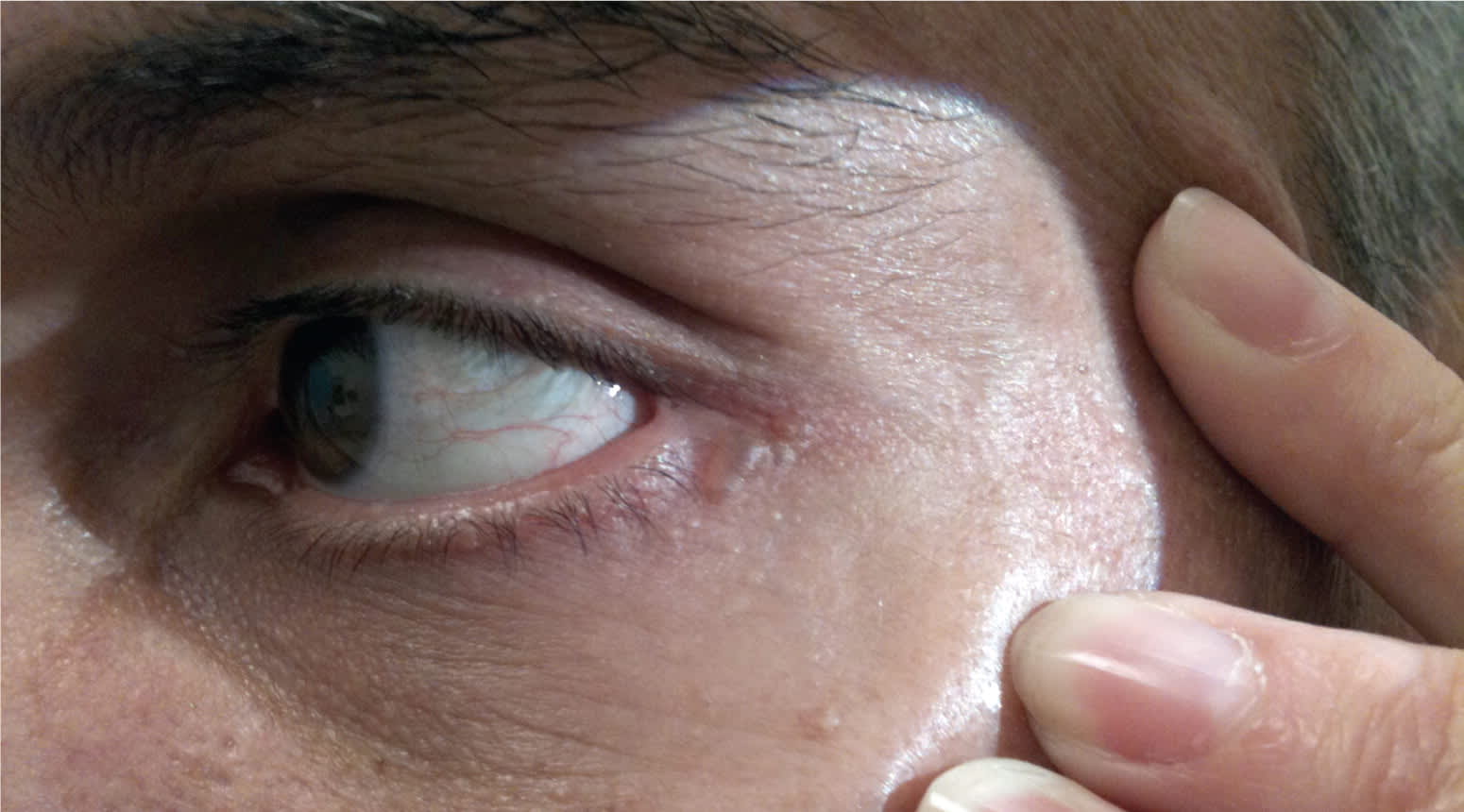
Examination revealed a 3- × 5-mm translucent, firm, dome-shaped, cystic papule with a bluish tint adjacent to the left lateral canthus (see accompanying figure). He had a few yellowish papules with central dells consistent with sebaceous hyperplasia on his forehead, but no other facial skin lesions.
Question
Based on the patient's history and physical examination, which one of the following is the most likely diagnosis?
A. Basal cell carcinoma.
B. Hidrocystoma.
C. Lymphangioma.
D. Sebaceous adenoma.
E. Syringoma.
Discussion
The answer is B: hidrocystoma. Hidrocystomas are benign cystic lesions affecting eccrine or apocrine sweat glands. They are thought to represent a cystic dilatation of intradermal sweat ducts, rather than a neoplastic proliferation.1 A hidrocystoma classically presents as a small, tense, thin-walled cyst near or on the eyelid margin.1 Hidrocystomas range from flesh-colored to a bluish or reddish hue, and may be solitary or multiple. Initial treatment for both eccrine and apocrine hidrocystomas involves a simple needle puncture2 or simple excision.
Basal cell carcinoma is the most critical lesion to rule out in the differential diagnosis of hidrocystoma lesions. A nodular basal cell carcinoma classically presents as a solid, pink to pearly white papule, often with prominent telangiectasias. Peripheral extension or central ulceration of the nodule is common.3 The bluish hue and cystic appearance of this patient's lesion, combined with a lack of growth, makes basal cell carcinoma less likely.
Lymphangiomas are rare, benign, lymphatic hamartomas that usually present in childhood or adolescence and are thought to be congenital. They are typically described as small (5 mm), translucent or hemorrhagic vesicles that are connected to deeper lymphatic or vascular channels.3 About 20 percent of lymphangiomas involve the orbit and ocular adnexa.4 Orbital lymphangiomas are rarely asymptomatic and usually present early in life with slowly progressive proptosis, displacement of the globe, ptosis, and restriction of eye movements.4
Sebaceous adenomas are benign tumors of sebaceous origin that may be solitary or multiple and are most often located on the head. Sebaceous adenomas appear as smooth, well-circumscribed, speckled, yellow papules that usually are less than 5 mm in diameter.5
Syringomas are benign tumors of the eccrine sweat duct that are more common in women older than 40 years. They usually are localized to the lower eyelids, but also appear on the forehead, neck, chest, abdomen, and vulva.3 Syringomas are small, solid, firm, flesh-colored dermal papules that are rarely solitary.6
Summary Table

| Condition | Characteristics |
|---|---|
| Basal cell carcinoma | Solid, pink to pearly white papule, often with prominent telangiectasias |
| Hidrocystoma | Solitary or multiple, small, tense, thin-walled cysts near or along the eyelid margin; flesh-colored to bluish or reddish hue |
| Lymphangioma | Small, translucent or hemorrhagic vesicles connected to deeper lymphatic or vascular channels |
| Sebaceous adenoma | Solitary or multiple, small, smooth, well-circumscribed, speckled, yellow papules |
| Syringoma | Small, solid, firm, flesh-colored dermal papules; rarely solitary |
