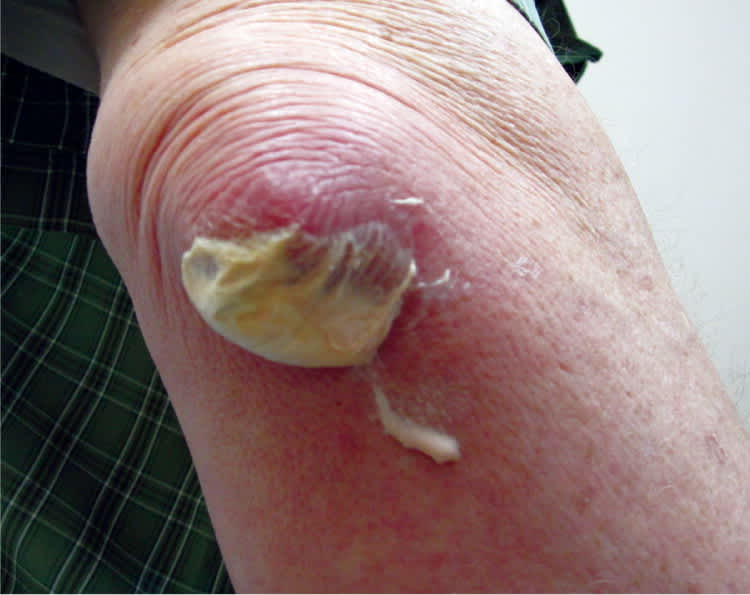
A 61-year-old man presented with a white pouch on his elbow. His elbow had been red, tender, and swollen for seven days before the pouch developed. He had no other symptoms and was afebrile, although he felt hot to the touch at the start of symptoms. He had no recent trauma to the joint. The patient had a history of gout, with the most recent attack several years prior.
Physical examination revealed fluid collection on the posterior aspect of the right elbow. The area was 2.5 × 5 cm in size and had a creamy white discharge (Figures 1 and 2). The surrounding area was erythematous, nontender, and warm to palpation. The patient had full range of motion. A wound culture showed no growth. His uric acid level was 8.3 mg per dL (494 μmol per L; normal = 3.7 to 8.6 mg per dL [220 to 512 μmol per L]).
Figure 1.

Figure 2.
Question
Based on the patient's history and physical examination findings, which one of the following is the most likely diagnosis?
A. Cellulitis.
B. Crystal-induced olecranon bursitis.
C. Septic olecranon bursitis.
D. Traumatic olecranon bursitis.
Discussion
The answer is B: crystal-induced olecranon bursitis. Olecranon bursitis is the most common superficial bursitis and can be caused by inflammation, infection, or trauma.1 It presents as a unilateral swelling over the proximal olecranon and most commonly affects men between 30 and 60 years of age.2 Approximately two-thirds of olecranon bursitis cases are noninfectious.3
Crystal-induced bursitis usually occurs in patients with a history of gout, although a history of trauma is also possible. The presence of gouty tophi increases the risk of developing olecranon bursitis. Physical examination reveals effusion, warmth, and erythema. There may be mild tenderness to the affected area, and the patient may have a low-grade fever. The bursal fluid can vary from straw-colored to bloody.4 Negatively birefringent, needle-shaped monosodium urate crystals can be visualized on polarized light microscopy. Treatment can include ice, compressive dressings, nonsteroidal anti-inflammatory drugs, and oral colchicine.
Cellulitis of the elbow is an infection of the skin through an abrasion or other break in the skin. The area will be erythematous, swollen, and warm to the touch. Patients may have a fever. Cellulitis is most commonly associated with Staphylococcus aureus or Streptococcus. Cellulitis of the elbow can progress to septic olecranon bursitis.
In septic olecranon bursitis, infection through breaks in the skin causes microorganisms to seed in the bursal sac, resulting in inflammation.2 The most common associated organism is S. aureus.3 Septic olecranon bursitis is more likely in patients with impaired immunity (e.g., those with diabetes mellitus, alcohol abuse, renal impairment, or malignancy).2 Patients usually present with fever, and the affected area is warm, erythematous, and tender. The tenderness is more pronounced with septic olecranon bursitis than with aseptic olecranon bursitis.3
Trauma can result in septic or aseptic bursitis. Even minor events, such as leaning on the elbow or repetitive motions, may result in traumatic bursitis,4 which is sometimes called “barfly elbow” or “student's elbow.” Contusions or abrasions to the elbow can cause swelling of the bursa.
Summary Table
| Condition | Characteristics | Test results |
|---|---|---|
| Cellulitis | Fever; erythema, swelling, warmth in affected area; no bursal fluid; possible history of trauma or skin abrasion/wound | Elevated serum WBC count, no bursal fluid |
| Crystal-induced olecranon bursitis | Usually afebrile; effusion, warmth, erythema, possibly mild tenderness in affected area; history of gout, possibly trauma | WBC < 1,000 per mm3 (1 × 109 per L) with a predominance of monocytes; bursal fluid glucose level 70 to 80 percent of serum level; negative Gram stain and culture results; negatively birefringent, needle-shaped monosodium urate crystals can be visualized on polarized light microscopy |
| Septic olecranon bursitis | Fever; warmth, erythema, severe pain in affected area; history of trauma or skin abrasion/wound | WBC > 10,000 per mm3 (10 × 109 per L) with a predominance of neutrophils, bursal fluid glucose level < 50 percent of serum level, positive Gram stain and culture results |
| Traumatic olecranon bursitis | History of trauma or skin abrasion/wound; history of repetitive pressure over the elbow | Negative Gram stain and culture results |
WBC = white blood cell.
