
A more recent article on common dermatologic conditions in skin of color is available.
Am Fam Physician. 2013;87(12):859-865
This is Part II of a two-part article on dermatologic conditions in skin of color. Part I, "Dermatologic Conditions in Skin of Color: Part I. Special Considerations for Common Skin Disorders," appears in this issue of AFP.
Patient information: See related handout on common conditions in skin of color, written by the authors of this article.
Author disclosure: No relevant financial affiliations.
Several skin conditions are more common in persons with skin of color, including dermatosis papulosa nigra, pseudofolliculitis barbae, acne keloidalis nuchae, and keloids. Dermatosis papulosa nigra is a common benign condition characterized by skin lesions that do not require treatment, although several options are available for removal to address cosmetic concerns. Pseudofolliculitis barbae occurs as a result of hair removal. Altering shaving techniques helps prevent lesions from recurring. In acne keloidalis nuchae, keloidal lesions are found on the occipital scalp and posterior neck. Early treatment with steroids, antibiotics, and retinoids prevents progression. A key part of the management of keloids is prevention. First-line medical therapy includes intralesional steroid injections. The distinct structure of the hair follicle in blacks results in hair care practices that can lead to common scalp disorders. For example, chemical relaxers decrease the strength of hair and may cause breakage. Better patient education, with early diagnosis and treatment, often leads to better outcomes.
Part I of this two-part article on dermatologic conditions in persons with skin of color discusses common conditions that require special consideration in this population.1 Part II reviews skin conditions relatively unique to skin of color, including dermatosis papulosa nigra, pseudofolliculitis barbae, acne keloidalis nuchae, keloids, and hair disorders.
| Clinical recommendation | Evidence rating | References | Comments |
|---|---|---|---|
| Medical management of pseudofolliculitis barbae includes a combination of topical steroids, benzoyl peroxide, topical retinoids, and topical antibiotics. | C | 9, 12, 14 | Observational studies and expert opinion |
| Topical retinoids, potent topical steroids, and topical antibiotics are initial therapies for acne keloidalis nuchae. | C | 14, 20 | Expert opinion and a small case study |
| Intralesional steroids are first-line therapy for keloids. | B | 25 | Meta-analysis of lower quality studies and expert opinion |
Dermatosis Papulosa Nigra
Dermatosis papulosa nigra is a common benign skin condition that occurs predominantly in dark-skinned persons (Table 12–8 ). It presents as 1- to 5-mm lesions appearing as multiple brown to dark-brown, dome-shaped papules on the face, neck, and trunk (Figure 1). Most patients incorrectly refer to the lesions as moles. The face is the most common location, with the malar and temple areas often involved. Usually there are no associated symptoms, although the lesions can occasionally be pruritic or become irritated.

The highest prevalence is in blacks, reportedly between 10% and 30%.2,3 However, this condition also affects Asians, Hispanic persons, and whites. Onset is typically after puberty, and lesions increase in number over time. The etiology is unknown. There appears to be a strong genetic predisposition; multiple family members often are affected, with more than 50% of patients reporting a family history of dermatosis papulosa nigra.2–4
Most patients present seeking reassurance that these lesions are benign. Treatment is not required, although if removal is sought, treatment options include scissor excision, laser therapy, electrodesiccation, curettage, cryotherapy, and microdermabrasion.4–8 Caution should be used in selecting a treatment modality because of the increased risk of postinflammatory hypo- or hyperpigmentation in persons with darker skin.
Pseudofolliculitis Barbae
Pseudofolliculitis barbae is an inflammatory condition typically involving the face and neck in persons with tightly curled hair (Table 29–12 ). It is commonly referred to as razor bumps and is recognized by follicularly-based erythematous and hyperpigmented papules and pustules. Although the pustules are usually sterile, secondary infections may develop. Postinflammatory hyperpigmentation, hypertrophic scars, and keloids often result.5
| Results from cut hairs penetrating the skin9 |
| Complete resolution is possible only with discontinuing hair removal10 |
| Applying proper shaving techniques can help decrease the extent of disease (Table 3) |
| Medical management includes topical steroids, benzoyl peroxide, topical antibiotics, and topical retinoids9,11,12 |
Pseudofolliculitis barbae affects men of African descent, with a prevalence of 45% to 85%.10 Hispanic men are the next most-affected group.9 In women, the face, axillae, and suprapubic areas are commonly involved. Pseudofolliculitis barbae develops after shaving or other forms of epilation, when cut hairs with an acute angle curl in on themselves and penetrate the skin, producing a foreign-body inflammatory reaction5,9 (Figure 2).

Treatment options include discontinuation of hair removal, destruction of the hair follicle, proper hair removal techniques, and medical management.13 To prevent recurrence, hair removal must be discontinued,10 which is often an impractical option. Therefore, recommended hair removal techniques can be used in combination with medical management11 (Table 35,9,10,14 ).
| Avoid a close shave, leaving hair at a length of 0.5 to 3 mm |
| Use clippers, a single-blade razor, or depilatories; if depilatories cause skin irritation, discontinue use |
| Shave in the direction of hair growth |
| Do not pull the skin taut while shaving |
| Loosen embedded hairs before shaving by brushing the neck, applying warm compresses, or gently rubbing with a towel |
| Avoid plucking |
Medical management includes use of a mild- to medium-potency topical steroid immediately after shaving, benzoyl peroxide or a topical antibiotic in the morning, and a mild retinoid (e.g., tretinoin [Retin-A] 0.025% or 0.05%) at night.12 If there are signs of infection, a short course of oral antibiotics is useful. Permanent hair reduction (e.g., laser hair removal, electrolysis) works by destroying the hair follicle and preventing hair growth.5,9,15–18 Glycolic acid and salicylic acid peels are also treatment options.
Acne Keloidalis Nuchae
Acne keloidalis nuchae is a progressive chronic folliculitis resulting in keloid-like papules and plaques on the occipital scalp (Table 414,19,20 ). Persons may present with 2- to 4-mm papules and pustules, typically at the occipital scalp and posterior neck, that may evolve to have a smooth, shiny appearance resembling keloids, often in a band-like distribution (Figure 3). Subcutaneous abscesses and draining sinuses may develop as well. Some patients experience pruritus and pain. Scarring alopecia in the involved area is common. These lesions are benign, but are often of cosmetic concern.
| Presents as papules, pustules, and plaques at the posterior scalp that are commonly associated with hair loss |
| First-line therapy includes use of topical antibiotics and potent topical steroids14 |
| Lesions with purulent drainage should be treated with oral antibiotics |
| Other therapies include intralesional steroids, topical and oral retinoids, imiquimod (Aldara), laser therapy, and surgical excision14,19,20 |

Acne keloidalis nuchae typically affects men, although women can be affected as well.21 The condition occurs in persons of all races but most commonly in men of African descent, followed by Hispanic, Asian, and white men. Persons affected are primarily postpubertal, and onset is typically before 50 years of age. It is of unknown etiology. Theories include chronic irritation and a pseudofolliculitis barbae–like foreign body reaction, secondary to skin penetration of closely shaven hairs and subsequent inflammation.14
Early treatment correlates with a good prognosis. Preventive measures include avoiding tight-fitting apparel that rubs the posterior hairline and not trimming the occipital hairline with a razor or clippers.10 Treatment includes potent topical steroids (class I and II), intralesional steroids, topical and oral antibiotics, topical and oral retinoids, imiquimod (Aldara), laser therapy, and surgical excision.14,19,20 Initial therapy begins with topical steroids, topical antibiotics, or both. Because treatment can be challenging, a combination of these therapies is usually indicated. Topical steroids in combination with topical antibiotics or retinoids can be effective in flattening lesions and decreasing symptoms. For draining or purulent lesions, bacterial culture permitting appropriate oral antibiotic selection is helpful.
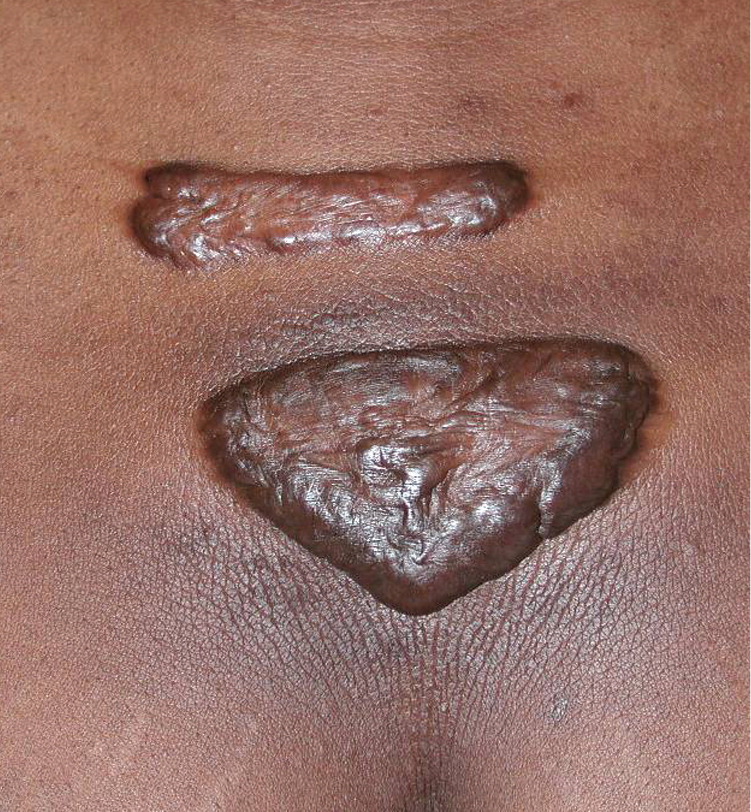
Keloids
Keloids are benign growths that represent an overgrowth of scar tissue at sites of trauma, such as acne, burns, surgery, ear piercing, tattoos, and infections. Keloids are smooth, shiny, and firm papules, plaques, and nodules. They tend to be red or pink with progressive hyperpigmentation (Figure 4). Common locations are ear lobes, jaw line, nape of the neck, scalp, chest, and back. Lesions are sometimes asymptomatic, but often are associated with pruritus, pain, and hypersensitivity. There is a higher incidence in blacks, Hispanic persons, and Asians. The most common ages at presentation are 10 to 30 years. Although the exact etiology of keloids is unknown, they are related to aberrant collagen production and breakdown in wound healing.22
Keloids are often confused with hypertrophic scars. Hypertrophic scars typically develop soon after the inciting trauma and are found on areas of the body with frequent motion, such as extensor surfaces.23 They are confined to the borders of initial injury and may regress. Conversely, keloids develop months to years after injury and are not usually located in areas of motion. Keloids extend beyond the borders of original injury, often progressing over time.
Patient education with an emphasis on prevention is essential. Guidelines for the prevention of keloids and hypertrophic scars include avoiding excessive movements that stretch the wound after undergoing procedures, and keeping wounds clean (Table 5).24 Patients with keloids often seek treatment for associated symptoms and cosmetic reasons. Although treatment can be challenging, early treatment offers the best outcome and many options are available. Often, multiple therapies are used in combination. A meta-analysis of several options, including intralesional steroids, interferon, fluorouracil, bleomycin, surgical excision, laser therapy, radiation, and cryotherapy, showed a 70% chance of improvement with treatment.25 Intralesional steroid injections (e.g., triamcinolone acetonide [Kenalog], 10 to 40 mg per mL) are first-line therapy. Triamcinolone acetonide at lower concentrations (10 mg per mL) may be used initially and titrated up based on response. In general, higher concentrations can be used safely in firmer, more elevated lesions. The possible adverse effects of atrophy, hypopigmentation, striae, and telangiectasias should be discussed with the patient before therapy, and the patient should be evaluated for these signs before each treatment. Lesions may be injected every four to eight weeks as indicated.
| Early treatment offers the best outcome |
| In persons prone to keloids, avoid unnecessary trauma to the skin (e.g., tattoos, piercings) |
| If surgery or other invasive procedures are required in a person prone to keloids,24 avoid excessive movements that stretch the wound, friction, and scratching; keep wounds clean to avoid infection and foreign body reactions |
| Use low concentrations of intralesional steroids for initial injections and titrate up as indicated; assess for skin atrophy and striae before each treatment |
| Intralesional steroid injections can be repeated every four to eight weeks Surgical excision alone has a high recurrence rate |
Other therapies exist, including silicone gel sheeting, pressure earrings, topical imiquimod, intralesional fluorouracil, intralesional bleomycin, surgical excision, laser therapy, and verapamil.22,24,26 Many of these therapies, particularly surgical excision, have a high rate of recurrence when used as monotherapy.
Hair Care Practices
Although no biochemical differences of hair have been found among persons of different ethnicities, there are notable differences in the shape of the hair follicle, leading to differences in texture, fragility, and manageability of hair. Persons of African descent have the greatest degree of curl and increased fragility. The hair is drier with less sebum production and can be difficult to comb in its natural state, resulting in many distinct hair care practices. These practices can lead to common scalp disorders27 (Table 628 ).
| Persons of African descent have various degrees of curl in their hair; mechanical fragility increases with higher degrees of curl |
| Because excessive hair washing can lead to breakage, less frequent shampooing is common; however, hair should be washed every one to two weeks to prevent buildup of styling product |
| Conditioning helps prevent hair fragility |
| Emollients are used for manageability but may cause acne or dermatitis28 |
| Chemical relaxers should be used no more often than every eight weeks |
| Heat can increase manageability, but in excess can result in hair damage |
| Styles such as braids and weaves may increase traction alopecia if there is excessive pull on the hair |
| Central centrifugal cicatricial alopecia is a common form of scarring hair loss and requires aggressive therapy and early intervention to prevent progression |
Although the rate is highly variable, many blacks shampoo their hair every one to two weeks.29,30 Depending on hair type, excessive washing causes the hair to be dry and brittle, and can increase breakage. However, infrequent washing may result in styling-product buildup and contribute to irritant dermatitis and seborrheic dermatitis.30 These can be reduced by shampooing and conditioning at least every two weeks. Emollients or hair grease used to increase manageability and protect the hair can sometimes contribute to acne, seborrheic dermatitis, and irritant dermatitis.28 Patients should be instructed to apply emollients only to the hair and limit contact with the face.
Hair straightening is accomplished by two methods: chemical alteration and heat.31,32 Chemical relaxers or perms break the disulfide bonds of the hair and must be used or performed at regular intervals to straighten the new hair that grows in. Overprocessing with frequent application of relaxers or reapplication to already straightened hair can result in breakage. Reapplication should occur no more than every eight weeks and be performed by a professional hair stylist. Adverse effects of relaxers include hair loss or breakage, color change, and chemical burns.31,33 Chemical burns occur when the relaxer is left on the scalp longer than the recommended treatment time. Heat, via pressing combs (hot combs) or flat irons, is an alternative method to straighten the hair. Pressing combs are metal combs heated by an external heating source and pulled through the hair to straighten. Hair breakage and thermal burns can occur. It is recommended that straightening with heat be performed only on clean hair and no more than every one to two weeks.
Traction alopecia (i.e., loss of hair from excessive pulling) often occurs at the frontal and temporal hair lines, and may result from tension placed on the hair with braids and weaves (Figure 5). Caution about the tightness and pull on the natural hair is advised. This is especially true for persons who use relaxers because their hair is already more vulnerable to breakage.34

An increasing number of patients are presenting with hair loss at the crown, which is known as central centrifugal cicatricial alopecia (Figure 6). This is the most common cause of permanent hair loss in blacks.35 Central centrifugal cicatricial alopecia is a scarring alopecia that begins at the crown and spreads outward. Women are more commonly affected than men. Mild pruritus, tenderness, and pain may be present. The etiology is unknown. Hair care practices, including use of relaxers, heat, and traction secondary to weaves and braids, have been suggested as causes.36,37 Although studies do not substantiate all of these associations,38 patients are encouraged to discontinue use of relaxers, limit traction, and decrease the amount of heat applied to the hair. No ideal treatment currently exists; however, options include topical and intralesional steroids with oral antibiotics. Early intervention is most effective.

Data Sources: A PubMed search was completed in Clinical Queries using the key terms skin of color, ethnic skin, dermatosis papulosa nigra, pseudofolliculitis barbae, acne keloidalis, keloids, and central centrifugal cicatricial alopecia. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. Also searched were the U.S. Preventive Services Task Force database, the Cochrane database, and the National Guideline Clearinghouse using the key terms skin, skin of color, hair, and skin cancer. Search dates: January to April 2011, and September to October 2011.
