
Am Fam Physician. 2014;89(6):473-475
Author disclosure: No relevant financial affiliations.
An 18-year-old man presented with a three-week history of a painful, nonpruritic, diffuse eruption involving the face. He had a history of atopic eczema and intermittent asthma flare-ups. There was no family history of atopy. He was not taking any medication. Treatment with oral prednisone one week earlier seemed to aggravate the condition.
Physical examination revealed a confluent, erythematous, edematous, hyperpigmented rash on the face. The eruption was composed of coalescent vesicles with honey-colored crusting (Figure 1). There were fissuring on the forehead and cheeks and open ulcerations in the nasomesial folds. There were no lesions elsewhere on the body.

Question
Discussion
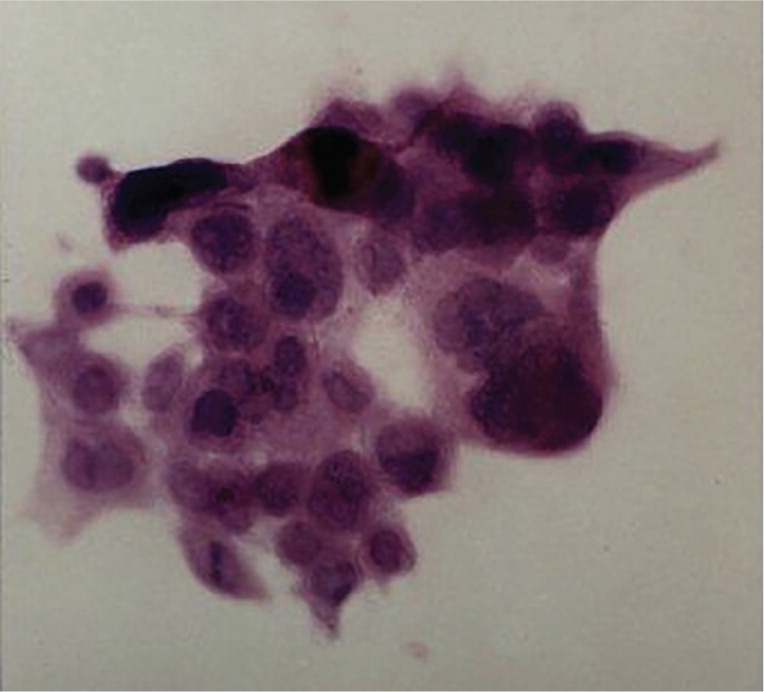
The answer is D: keratitis. The sudden onset of a widespread blistering facial rash in a patient with atopic eczema is suggestive of eczema herpeticum (Kaposi varicelliform eruption). This condition is commonly caused by herpes simplex viruses 1 and 2.1 A disrupted skin barrier from atopic or irritant dermatitis or Darier-White disease, coupled with local immune dysfunction, facilitates the spread of the virus.2 Other predisposing factors include a history of elevated immunoglobulin E levels and treatment with corticosteroids.3 Eczema herpeticum should be considered in patients with sudden onset of a widespread, blistering rash. Tzanck testing showing multinucleated giant cells (Figure 2) is confirmatory. Viral culture, polymerase chain reaction testing, direct immunofluorescence, and histologic examination can also be used to confirm the diagnosis.4
Herpetic keratitis is a major ophthalmologic complication of eczema herpeticum. Ophthalmologic consultation is recommended when the patient has red or irritated eyes.2 Vesicles with purulent drainage may occur on the eyelids. Ocular pain, photophobia, foreign object sensation, and tearing are common.5 Recurrent herpetic keratitis is a primary cause of acquired blindness in the industrialized world.6
Arthritis that is migratory or transient is a common early symptom of systemic lupus erythematosus.5 The acute cutaneous manifestation of lupus is the butterfly facial erythema, an eruption that begins in the malar area and the bridge of the nose, sparing nasolabial folds. Bullous lesions occur as grouped vesicles, usually on sun-exposed areas (e.g., head, neck, arms). Vesicles are not typically seen on the corneal surface.
Epididymitis is a common scrotal inflammatory condition and can be a complication of Chlamydia trachomatis or Neisseria gonorrhoeae infection.5 Typical symptoms include testicular pain, scrotal nodules, urethral discharge, and dysuria, although some cases are asymptomatic. Pathogens such as varicella and herpes simplex virus cause orchitis as a result of disseminated disease in severely immunocompromised persons.5
Group A beta-hemolytic streptococcal skin infections are complicated by poststreptococcal glomerulonephritis in about 2% to 5% of patients.5 Impetigo typically occurs in children younger than six years and is characterized by discrete, sharply demarcated vesicles with rapid progression to honey-colored crusting.5
Meningitis can occur in patients with primary genital herpes simplex virus 2 infection. Overall, herpes simplex virus 2 is responsible for less than 1% to 3% of all cases of aseptic meningitis.7 Herpes simplex virus 1 infection is rarely associated with aseptic meningitis. Patients with meningitis present with signs of meningeal irritation, including nuchal rigidity, headache, and stiffness. Anorexia, vomiting, and a nonspecific rash sometimes occur.
| Condition | Characteristics |
|---|---|
| Arthritis | Migratory or transient arthritis is a common early sign of systemic lupus erythematosus |
| Butterfly facial erythema; bullous lesions of systemic lupus erythematosus occur as grouped vesicles, usually on sun-exposed areas (e.g., head, neck, arms) | |
| Epididymitis | Can be a complication of Chlamydia trachomatis or Neisseria gonorrhoeae infection |
| Testicular pain, scrotal nodules, urethral discharge, and dysuria, although some cases are asymptomatic | |
| Glomerulonephritis | Can be a complication of group A beta-hemolytic streptococcal skin infections; typically occurs in children younger than six years |
| Impetigo typically occurs in children younger than six years and is characterized by discrete, sharply demarcated vesicles with rapid progression to honey-colored crusting | |
| Keratitis | Major morbidity associated with eczema herpeticum |
| Ocular pain, photophobia, foreign object sensation, and tearing; sudden onset of a widespread, blistering facial rash in persons with atopic eczema | |
| Meningitis | Primary genital herpes simplex virus 2 infection can lead to aseptic meningitis |
| Meningeal irritation, including nuchal rigidity and headache; anorexia, vomiting, and nonspecific rash sometimes occur |
