Nearly 4,000 drowning deaths occur annually in the United States, with drowning representing the most common injury-related cause of death in children one to four years of age. Drowning is a process that runs the spectrum from brief entry of liquid into the airways with subsequent clearance and only minor temporary injury, to the prolonged presence of fluid in the lungs leading to lung dysfunction, hypoxia, neurologic and cardiac abnormalities, and death. The World Health Organization has defined drowning as “the process of experiencing respiratory impairment from submersion/immersion in liquid.” Terms such as near, wet, dry, passive, active, secondary, and silent drowning should no longer be used because they are confusing and hinder proper categorization and management. The American Heart Association's Revised Utstein Drowning Form and treatment guidelines are important in guiding care, disposition, and prognosis. Prompt resuscitation at the scene after a shorter duration of submersion is associated with better outcomes. Because cardiac arrhythmias due to drowning are almost exclusively caused by hypoxia, the resuscitation order prioritizes airway and breathing before compressions. Prevention remains the best treatment. Education, swimming and water safety lessons, and proper pool fencing are the interventions with the highest level of current evidence, especially in children two to four years of age. Alcohol use during water activities dramatically increases the risk of drowning; therefore, abstinence is recommended for all participants and supervisors.
Drowning kills nearly 4,000 persons in the United States and more than 300,000 persons worldwide every year.1 For U.S. children between one and four years of age, drowning has surpassed motor vehicle crashes as the most common injury-related cause of death at 2.6 per 100,000 persons annually.2 Despite this significant health burden, public health initiatives have lagged because of lack of standardization in definitions and reporting.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| Alcohol greatly increases drowning risk and should not be used when participating in or supervising water activities. | C | 10–13 |
| In drowning victims, the order of resuscitation efforts should be airway, breathing, and compressions (ABC), rather than compressions, airway, and breathing (CAB), because cardiac arrhythmias are almost exclusively secondary to hypoxia. | C | 23 |
| Educational programs, swimming and water safety lessons, and pool fencing may be effective strategies in preventing childhood drowning. | B | 12, 13, 29 |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
Definition
Before the first World Congress on Drowning (WCOD) in 2002, public health surveillance, research, and policy on drowning were impeded by a lack of clear terminology.3 Highlighting this problem, a systematic review of the literature from 1966 to 2002 found at least 33 different definitions for drowning incidents.4 The WCOD was organized largely to remedy this issue. The WCOD developed consensus guidelines using the Utstein principles—a term coined from a series of meetings held at Utstein Abbey in Stavanger, Norway, to clarify the nomenclature associated with out-of-hospital cardiac arrests.4 The guidelines applied the same principles to clarify definitions, terminology, and data sets used in the epidemiology and treatment of drowning.5 Following extensive discussion and debate, the World Health Organization agreed on the following definition: “Drowning is the process of experiencing respiratory impairment from submersion/immersion in liquid.”3
Terms such as near, wet, dry, passive, active, secondary, and silent drowning should not be used because they can be confusing and ultimately hinder classification or management.3 The Utstein approach simplified the classification of drowning outcomes to only three domains: death, morbidity, and no morbidity.3
Epidemiology
Despite declines in the death and hospitalization rates from drowning over the past decade, it remains the top injury-related concern in children.2,6,7 Approximately 5,800 persons are treated in U.S. emergency departments each year for submersion or drowning injuries, with one-half of those patients requiring hospital admission.6,8,9 Permanent neurologic sequelae, such as persistent vegetative state or spastic quadriplegia, occur in 5% to 10% of childhood drowning cases.10
The typical location of drowning varies depending on age. Children younger than four years are more likely to drown in a swimming pool, whereas adults are more likely to drown in a natural body of water (Figure 1).6 A systematic review found drowning to be the most common cause of recreational aquatic activity death in persons 15 years or older; 30% to 70% of drowning fatality victims had alcohol in their bloodstream.11 Even small amounts of alcohol increase the risk of drowning, and this risk increases with the amount of alcohol consumed.10–13
Figure 1.
Distribution of fatal and nonfatal drownings, by location and age group from the National Vital Statistics System and National Electronic Injury Surveillance System—All Injury Program, United States, 2005–2009.
Adapted from Centers for Disease Control and Prevention. Drowning—United States, 2005–2009. MMWR Morb Mortal Wkly Rep. 2012;61(19):346.
Pathophysiology and Clinical Presentation
Understanding the drowning process bolsters accurate diagnosis, treatment, and prognosis. Initially, fluid enters the oropharynx and is cleared, if possible. If clearing is not possible, conscious breath holding ensues. Eventually, the internal drive to inspire becomes insurmountable, and fluid enters the airways, stimulating cough or laryngospasm. If the drowning process continues, a number of events may occur, such as fluid and electrolyte shifts, alveolar dysfunction, and hypoxia.14,15 These may trigger further deterioration with pulmonary edema, decreased lung compliance, and bronchospasm.14,15 Cardiac deterioration develops after seconds to minutes of hypoxia, typically progressing from tachycardia to bradycardia, pulseless electrical activity, and asystole.15–17
Evaluation and Treatment
The Utstein approach to the evaluation of drowning victims not only standardizes reporting and data collection but also provides guidance for the history, physical examination, and appropriate management (eFigure A).
eFigure A. Revised Utstein Drowning Data Form
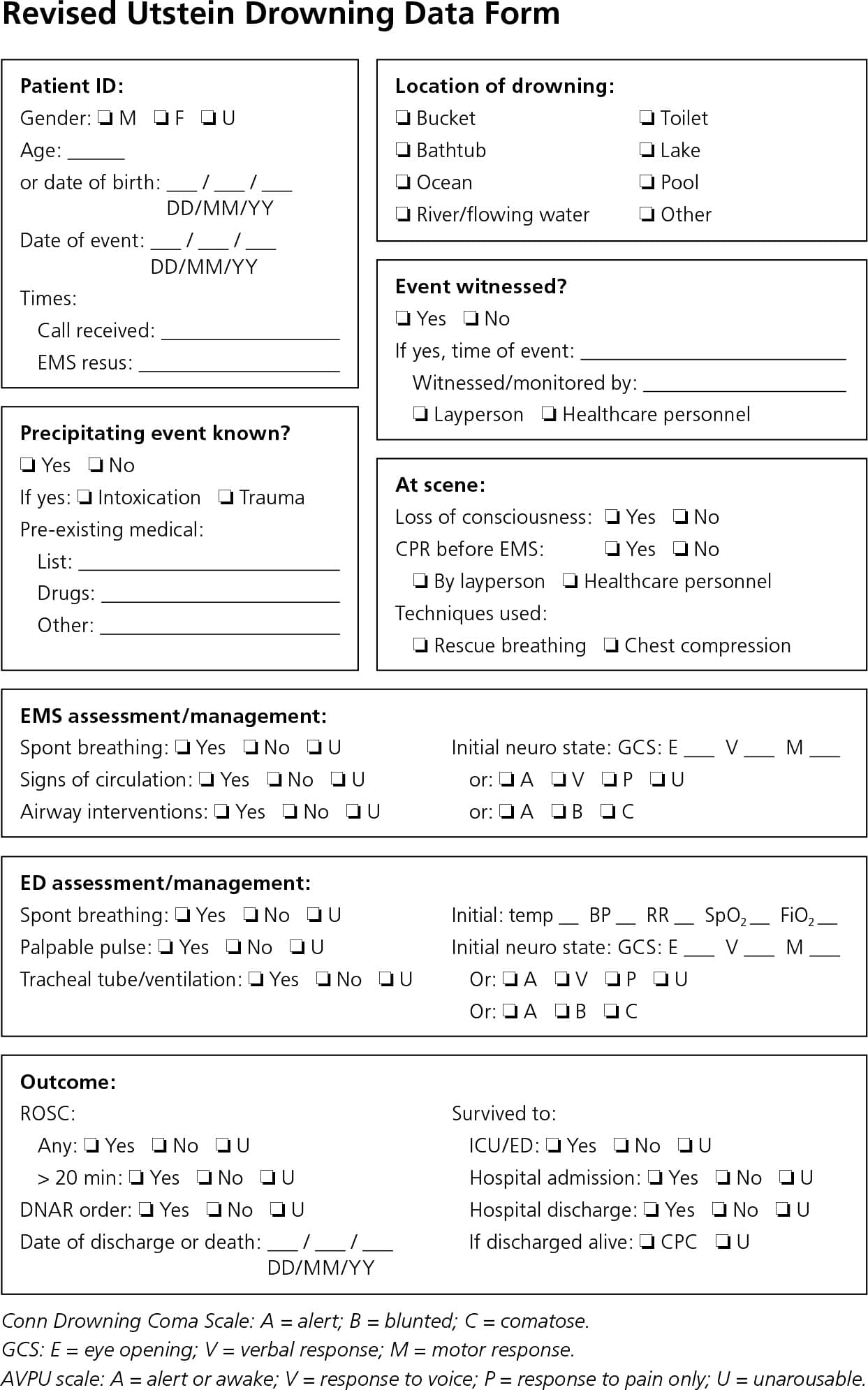
Revised Utstein drowning data form. (BP = blood pressure; CPC = cerebral performance category; CPR = cardiopulmonary resuscitation; DNAR = do not attempt resuscitation; ED = emergency department; EMS = emergency medical services; FiO2 = fraction of inspired oxygen; GCS = Glasgow Coma Scale; ICU = intensive care unit; ROSC = return of spontaneous circulation; RR = respiratory rate; SpO2 = arterial oxygen saturation; U = unknown.)
Reprinted with permission from Idris AH, Berg RA, Bierens J, et al.; American Heart Association. Recommended guidelines for uniform reporting of data from drowning: the “Utstein style.” Circulation. 2003;108(20):2570. http://circ.ahajournals.org/content/108/20/2565.long.
HISTORY
Details of the drowning event guide treatment and determine prognosis. Younger patients tend to have better outcomes.18 Submersion for six minutes or longer is associated with a significantly poorer prognosis. When considering open water drowning victims with good outcomes (i.e., did not die or experience severe neurologic sequelae), 88% were submerged less than six minutes vs. 7.4% of victims with six to 10 minutes of submersion.18 In-water resuscitation, where several rescue breaths are given by trained lifesaving personnel while still in the water, is associated with shorter duration of anoxia and a higher rate of survival.19 Lack of adequate training, open-water conditions, distance to shore, water depth, equipment availability (e.g., flotation devices), and a person's features (e.g., injury, obesity) may limit the feasibility of in-water resuscitation.19
Cold water submersion was previously considered neuroprotective because of decreased metabolic demands of hypothermia and the diving reflex. Case reports described young victims with prolonged submersion in very cold water who survived neurologically intact.20,21 However, it has been determined that water temperature has no correlation with overall outcome.18 Contrary to popular belief, fresh vs. saltwater aspiration makes no difference in the degree of lung injury.15
Unless the victim has experienced a diving or boating accident or has fallen from a height, cervical spine immobilization is unnecessary because only 0.5% of drowning victims have a cervical spine injury.22
PHYSICAL EXAMINATION AND INITIAL TREATMENT
A drowning classification system has been established to classify victims at the rescue scene based on the clinical parameters of respirations, pulse, pulmonary auscultation, and blood pressure14,17 (Figure 217 ).
Figure 2. Classification System of Drowning Grades to Guide Risk Stratification and Management
Classification system of drowning grades to guide risk stratification and management. (ABC = airway, breathing, and compressions; CPR = cardiopulmonary resuscitation.)
Reprinted with permission from Szpilman D, Bierens JJ, Handley AJ, Orlowski JP. Drowning. N Engl J Med. 2012;366(22):2105.
Attention to airway, breathing, and compressions (ABC) in that order (compared with the modern advanced cardiac life support guidelines' compressions, airway, and breathing [CAB]) is paramount because any cardiac arrhythmias are almost exclusively secondary to hypoxia.23 A patient who is not breathing or has a Glasgow Coma Scale score less than 8 should be intubated and given ventilatory support.14 Conscious drowning victims with rales in some or all pulmonary lung fields require supplementary oxygen and evaluation in the emergency department.14,17 A victim who is still on the scene, has no other medical complications, and demonstrates clear lung fields (with or without a cough) does not automatically require further medical attention.14,17 This represents more than 94% of lifeguard rescues.14,17
Vomiting occurs in 30% to 85% of drowning victims because of swallowing large amounts of water and positive pressure ventilation during resuscitation.19,24 Aspiration of gastric contents portends worse lung injury.
DIAGNOSTIC EVALUATION
Although certain diagnostic evaluations start at the scene and may progress to an emergency department, the overall breadth of diagnostic workup is limited and primarily focuses on respiratory function. If hypothermia is a concern, infrared thermometric devices should not be used to determine core temperature because they register falsely lower body temperatures in victims whose heads have been submerged.25 On arrival to the emergency department, clinical impression should guide laboratory studies. Serum electrolyte, hemoglobin, and hematocrit levels are typically in normal ranges and measurement is not beneficial.17,26 An initial chest radiograph may be unremarkable even if significant lung injury has occurred, or, conversely, pneumonia may be overdiagnosed because of water in the lungs.27,28 Drowning victims with suspected head or neck trauma should undergo computed tomography of the head and cervical spine.22 For drowning victims in cardiac arrest, a nonshockable rhythm (asystole or pulseless electrical activity) is more common than in nondrowning cardiac arrest victims.16
Prevention
Drowning is rarely caused by a single factor; therefore, prevention strategies should not be pursued in isolation.12 Prevention methods target the aforementioned epidemiologic concerns and can be divided into physical, behavioral, medical, and community/government areas of interest (Table 110–13,17,29–33 ). Although rigorous studies with high-level evidence are lacking, there is some evidence supporting educational programs, swimming and water safety lessons, and pool fencing in the prevention of drowning, especially in children two to four years of age.12,13,29 Residential pool safety measures are highlighted by the American Academy of Family Physicians in its clinical policy statement at https://www.aafp.org/about/policies/all/residential-pool.html. With adequate supervision, swimming instruction, and public education measures, it is estimated that 85% of drownings can be prevented.30
Table 1. Drowning Prevention Methods
| Method | Comments | ||||
|---|---|---|---|---|---|
| Physical | |||||
| Pools | |||||
| Fencing | Odds ratio for drowning in a fenced vs. an unfenced pool = 0.27 (95% confidence interval, 0.16 to 0.47)29 | ||||
| Four-sided fencing completely surrounding pool (not attached to house on one side) | |||||
| Gates should open away from the pool, be self-closing and self-latching, with the latching mechanism at least 58 inches above the ground | |||||
| Fence composition should not be climbable (e.g., not chain link) | |||||
| Fence should be at least 4 feet high with no more than 4 inches between vertical aspects and no more than 4 inches between the bottom of the fence and the ground | |||||
| Drain covers, safety vacuum release systems, multiple drains to displace pressure | Prevents entrapment and entanglement of hair or body parts; other filter techniques that provide pressure venting should be implemented | ||||
| Rescue equipment | U.S. Coast Guard–approved water rescue equipment (such as a reaching pole or shepherd's crook and life buoys) should be readily available poolside, in addition to a working telephone | ||||
| Pool alarms (multiple types, such as floating, subsurface, and wristband alarms) | No evidence that alarms are of benefit; may provide a false sense of security; not a substitute for adequate supervision or adequate pool fencing | ||||
| Personal flotation devices | According to a 2008 report from the U.S. Coast Guard, 91% of drowning victims (464 of 510) were not wearing personal flotation devices31 | ||||
| There is little evidence on effectiveness, but use likely decreases morbidity and mortality; proper use is based on the individual and the setting | |||||
| See U.S. Coast Guard guidelines at http://www.uscg.mil/hq/cg5/cg5214/pfdselection.asp | |||||
| Floatable swimming aids | Not approved as personal flotation devices; do not replace adequate supervision | ||||
| Air-containing types can deflate | |||||
| Bath stands | Drownings associated with bath stand use were caused by product defect in < 10% of cases33 | ||||
| May give caregivers the false perception that the infant needs less attention; cannot substitute for adequate direct supervision | |||||
| Behavioral | |||||
| Avoid alcohol use | 30% to 70% of adults who die from drowning have positive blood alcohol levels11 | ||||
| Discourage the use of alcohol or other drugs for all boaters and participants in water recreation | |||||
| Adults supervising children should not be using alcohol or drugs | |||||
| CPR | Immediate on-the-scene care is important for survival | ||||
| All adults and caregivers should be trained in CPR and understand the rationale for using the ABC order of resuscitation (not the CAB order) | |||||
| Supervision | |||||
| Lifeguards | Encourage use of water recreation areas staffed by lifeguards with certification in CPR | ||||
| Adults/caregivers | Knowledge of CPR should be mandatory for supervising children | ||||
| Direct supervision should be employed with any age swimmer; adult “water watchers” should avoid distracting activities | |||||
| Touch supervision must take place with nonswimmers; adult should be in the pool and within arm's reach of nonswimmer at all times | |||||
| Avoid rip currents | Learn characteristics of rip currents (e.g., reverse bubbles moving away from beach, broken waves between sandbars) | ||||
| Encourage use of beaches with lifeguards and heed warnings of posted surf conditions | |||||
| To escape, do not battle current; swim perpendicular to current (parallel to shore) until cleared from rip current and then swim at an angle, away from the current and toward the shore | |||||
| For safety tips about rip currents, see http://www.ripcurrents.noaa.gov/ | |||||
| Open bodies of water and other natural swim areas | |||||
| Approach water with an unknown depth and/or hazards with caution | Even in clear water, depths may be uncertain, so entering feet first the first time is advised | ||||
| Assess for currents | Swift currents can trap persons underneath rocks, trees, or other debris, and can overwhelm even strong swimmers | ||||
| Standing water | |||||
| Monitor water-containing objects | Buckets, inflatable pools, and natural standing water should never be left unattended; buckets and inflatable pools should be emptied when not in use | ||||
| Restrict toddlers' access to bathrooms and toilets with childproof latching systems | |||||
| Education | |||||
| Swimming and water safety lessons | Possibly effective in children two to four years of age | ||||
| American Academy of Pediatrics supports swimming lessons for children four years and older | |||||
| Medical | |||||
| Monitor children with seizure disorders | Children with seizure disorders should always have direct supervision when swimming or bathing | ||||
| Showering is preferable to bathing when supervision cannot take place because of privacy concerns | |||||
| Monitor children with autism spectrum disorder and cardiac channelopathies (long QT syndrome and catecholaminergic polymorphic ventricular tachycardia) | There is slight evidence that children with these disorders have increased rates of drowning and thus may require increased supervision | ||||
| Community/government | |||||
| Office-based interventions | Can be implemented by physicians and support staff | ||||
| Identify families with access to residential pools for targeted drowning prevention counseling | |||||
| Ensure adequate counseling and support services for drowning victims | |||||
| Legislation to prevent drowning | Safe pool fencing | ||||
| Proper staffing of pools or public swimming areas with CPR-certified lifeguards | |||||
| Strict boating laws regarding alcohol consumption | |||||
| Drowning awareness campaigns; educational materials | CPR training | ||||
| Swimming lessons | |||||
| Drowning prevention techniques | |||||
ABC = airway, breathing, and compressions; CAB = compressions, airway, and breathing; CPR = cardiopulmonary resuscitation.
Information from references 10 through 13, 17, and 29 through 33.
Data Sources: A PubMed search was completed in Clinical Queries using the key terms drowning and near-drowning. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. Also searched were the Agency for Healthcare Research and Quality evidence reports, Essential Evidence Plus, the Cochrane database, Database of Abstracts of Reviews of Effects, the Trip database, and the Family Physicians Inquiries Network content. Search dates: September 19, 2014, and January 23, 2016.
The views expressed are the authors' and do not reflect the official policy or position of the U.S. government, Department of the Navy, or Department of Defense.
