
Am Fam Physician. 2016;93(11):945-946
Author disclosure: No relevant financial affiliations.
A 10-year-old boy presented with a rash on both hands that had been present for at least several weeks. He had not worn any new gloves or other clothing. He had received a new video game at Christmas about five months prior and had played it for at least three to four hours every day since.
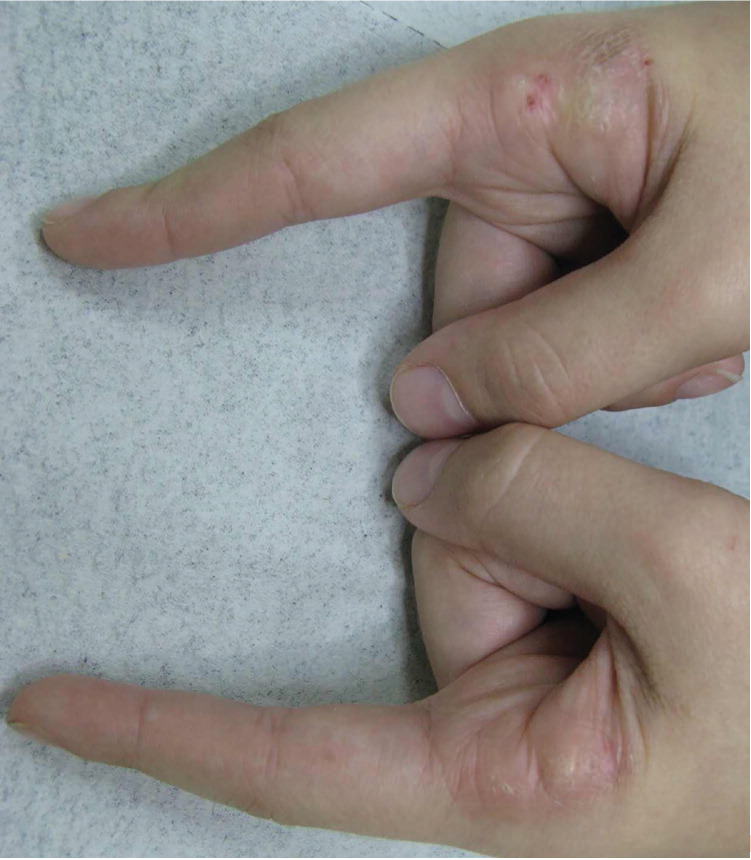
On physical examination, he was not in distress. There were hyperkeratotic plaques on the lateral aspect of both of his index fingers (Figure 1). The lesions were symmetric, lichenified with erosions, and painful. The rest of the dermatologic examination was unremarkable.
Question
Discussion
The answer is A: frictional hyperkeratotic hand dermatitis. The patient's lesions developed at the sites of direct contact with his video game controller, and the diagnosis was made based on the repetitive friction and trauma caused by overuse of the video game. He was successfully treated by significantly reducing his video game use and applying topical emollients.
With the increased use of computers and electronic devices by persons of all ages over the past 20 years, new manifestations related to repetitive mechanical activities may occur, affecting superficial structures, such as the skin, and less commonly deeper structures, such as nerves and tendons. Frictional hyperkeratotic hand dermatitis develops as a result of repetitive mechanical friction, trauma, vibration, or pressure. Several terms have been used to describe injuries from overuse of electronic devices, including “Nintendonitis,” “Wiitis,” and “Playstation thumb.”
Irritant contact dermatitis is a localized inflammatory response to physical, environmental, or chemical agents. It usually presents as erythema, erosions, and scaling and may cause pruritus or a burning sensation. Mild symptoms result from prolonged or repeated exposure to the irritants. Strong chemicals may produce a direct reaction similar to that of a thermal burn.1
Palmoplantar keratodermas are a heterogeneous group of disorders with hyperkeratotic thickening of the palms and soles.2 These disorders may be hereditary or acquired. The diffuse form has a thick, symmetric hyperkeratosis involving the entire palm and sole. The focal form has hyperkeratotic lesions at sites of recurrent friction, mainly on the feet. The punctate form is characterized by punctate keratotic papules on the palms and soles.3
Psoriasis is a chronic, immune-mediated inflammatory disease.4 It presents as erythema, thickening, and scaling of the skin. It may be accompanied by deep, painful fissures or palmoplantar pustulosis.
Tinea manuum is a superficial, noninflammatory dermatophyte infection of the hand. It usually presents as diffuse, dry, scaling hyperkeratotic lesions, although vesicular, exfoliating, erythematous, annular lesions on the dorsal surface of the hand have also been reported. Unilateral tinea manuum is associated with moccasin-type tinea pedis or onychomycosis, a pattern sometimes referred to as two feet, one hand disease.5
| Condition | Characteristics | Etiology |
|---|---|---|
| Frictional hyperkeratotic hand dermatitis | Hyperkeratotic plaques of the hands that are symmetric, lichenified with erosions, and painful | Repetitive mechanical friction, trauma, vibration, or pressure |
| Irritant contact dermatitis | Erythema, erosions, and scaling; possibly pruritus or a burning sensation | Localized inflammatory response to physical, environmental, or chemical agents |
| Palmoplantar keratodermas | Diffuse form: thick, symmetric hyperkeratosis involving the entire palm and sole | Hereditary (autosomal recessive, autosomal dominant, or X-linked), or acquired |
| Focal form: hyperkeratotic lesions at sites of recurrent friction, mainly on the feet | ||
| Punctate form: punctate keratotic papules on the palms and soles | ||
| Psoriasis | Erythema, thickening, and scaling of skin; deep, painful fissures or palmoplantar pustulosis | Immune-mediated inflammatory disease |
| Tinea manuum | Diffuse, dry, scaling hyperkeratotic lesions; possibly vesicular, exfoliating, erythematous, annular lesions on the dorsal surface of the hand | Superficial, noninflammatory dermatophyte infection |
