
Supreme Court: HMO financial incentives OK, Congress must act
The Supreme Court ruled unanimously last month that patients cannot sue their HMOs in federal court for giving physicians financial incentives to reduce treatment costs (Pegram et al v Herdrich). The court found that such financial incentives do not breach health plans' fiduciary duties under the 1974 Employee Retirement Income Security Act (ERISA). In fact, wrote Justice David Souter in the court opinion, such incentives are necessary because “no HMO organization could survive without some incentive connecting physician reward with treatment rationing.” Such suits would mean “nothing less than elimination of the for-profit HMO,” a structure Congress has promoted for 27 years, said Souter. He suggested that a legislative solution may be preferable to a judicial one.
Rep. Charles Norwood, R-Ga., interpreted the court's opinion as a challenge to Congress to institute managed care reform. “The justices are shouting at the top of their lungs for us to act,” he said, in the June 13 New York Times.
The Supreme Court's decision overturned a 1998 decision by the 7th U.S. Circuit Court of Appeals. The ruling leaves open the possibility of suing HMOs in state courts that have applicable laws, and it does not affect patients' rights to sue hospitals and physicians at the state level for malpractice. The plaintiff in this case was awarded $35,000 in damages for medical malpractice. Her appendix ruptured, causing peritonitis, after her physician delayed diagnostic tests for eight days so they could be performed at a facility the physician had a financial incentive to refer to.
Meanwhile, the congressional conference committee charged with creating a compromise patients' bill of rights has yet to complete its task after nearly four months of debate. In an attempt to stir progress, Sen. Edward Kennedy, D-Mass., forced the Senate to vote on the House's version of the patients' bill of rights, passed last fall, by adding it to a defense spending bill on June 8. It was defeated by three votes.
Downcoding
Delivering its quarterly report to Congress last month, the Medicare Payment Advisory Commission (MedPAC) said it has, for the first time, found evidence of significant downcoding by physicians, hospitals and other health care providers. MedPAC suggested that the coding problem could be due, in part, to heightened efforts to combat Medicare fraud.
Meanwhile …
The Office of Inspector General (OIG) has issued draft compliance-program guidelines intended to help solo and small group practices avoid Medicare and Medicaid fraud and abuse. The guidelines were published in the June 12 Federal Register. Although the OIG is urging all practices to implement such programs, it says it “believes the great majority of physicians are honest.” In fact, at a recent HCFA regional office meeting in Kansas City, Mo., officials noted that of the 600,000 physicians in the United States, the federal government prosecuted only 43 last year, all of them egregious cases.
Switching doctors
Americans change their physicians and other health care providers more often because of personal preference than because of health plan rules, according to two surveys by The Center for Studying Health System Change. The studies show that of those changing providers 40 percent did so for convenience, to improve their care or to see a particular doctor. Only 20 percent changed providers because their health plan required them to do so.
Physician report cards
In the largest study of its kind, the National Research Corporation plans to compile physician quality report cards on the nation's 143,000 primary care physicians. The study will require 15 million households to be surveyed, beginning this year with Cincinnati and Portland. Those results should be available in October.
High prescription costs
The cost of prescription drugs for employers increased 15.9 percent last year, according to Merck-Medco's Drug Trend 2000 Report. Drug costs more than doubled from 1995 to 1999, in part because more people are taking prescription drugs, people are taking them for longer periods of time and newer, more expensive drugs are replacing older, cheaper ones, says the report.
Columbia no more
Shortly after agreeing to pay the government $745 million to settle the largest Medicare fraud investigation in history, Columbia/HCA announced it will now be known as HCA – The Healthcare Company. This follows three years of negative publicity, during which “Columbia — the name and the company —became almost synonymous with an aggressive health-care culture which had led to the fraud scandal,” the May 26 New York Times reports.
Unhealthy Americans
A new way to calculate “healthy life expectancy,” developed by the World Health Organization (WHO), ranks the United States 24th, behind most European countries, Canada, Australia and Japan, which ranked first. WHO attributes the United States' low ranking to high rates of tobacco-related disease, heart disease, homicide and injury. “Basically, you die earlier and spend more time disabled if you're an American,” says Christopher Murray, MD, PhD, director of WHO's global program on evidence for health policy.
Family physician income, workload
Family physicians' income averaged $134,000 last year (before taxes, not including benefits), according to a recent survey by the AAFP. The average workload associated with that income is shown in the graph below. The data does not take into account complexity of visits and other factors affecting physician productivity.
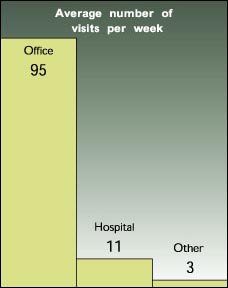
Source: AAFP, Practice Profile I survey, May 2000
GOP cancels vote to give physicians collective bargaining power
Facing strong opposition from insurance companies and from within their own party, House Republican leaders recently pulled from the House floor legislation that would allow doctors to bargain collectively with insurance companies. The bill proposes to give physicians in private practice a three-year exemption from antitrust laws. More than half of all U.S. doctors would be affected.
Sponsored by Rep. Tom Campbell, R-Calif., the bill has considerable bipartisan support and is backed by the AMA, but some groups, such as the American Association of Health Plans, say the proposal would lead to higher medical costs for consumers and would give physicians too much power.
One coalition working to defeat the bill has waged an aggressive media campaign in Washington, D.C., saying, “Doctor cartels are bad medicine for patients.”
The Campbell bill may be rescheduled for a vote later this year.
Medical-error prevention gains attention
The recent Institute of Medicine study estimating that 98,000 Americans die every year because of medical errors has given rise to a growing number of public and private initiatives that aim to reduce mistakes. Here are just a few:
- The Department of Veterans Affairs has hired NASA to establish a system that will allow workers at the 172 VA medical centers to report medical mistakes without fear of penalty, according to Reuters Health. NASA will use the Aviation Safety Reporting System as a starting point for developing the new system.
- Cedars-Sinai Medical Center in Los Angeles recently arranged a penmanship workshop for medical staff to reduce prescription-related errors, reports the Washington Post. Two handwriting specialists led the course, which focused on “box-and-stick” style letters. The course was elective, but the chief of staff encouraged the participation of several dozen doctors identified by nurses as having particularly poor penmanship.
- The Healthcare Leadership Council, a group of CEOs from various disciplines within the health care system, has created a patient safety task force, which it says will work to change both the culture and the systems that lead to mistakes. A top priority for the task force will be the issue of naming, labeling and packaging of medications, which it views as a major source of error.
Quote. Endquote.
“The health care backpack in my opinion is full of a lot of useless assumptions so old and so often repeated that they become facts from the mouth of Hippocrates and to question them risks one's relationships with co-professionals, but we are going to have to question them.”
Don Berwick, MD, MPP, president and CEO of the Institute for Health-care Improvement (IHI) and clinical professor of pediatrics and health care policy at Harvard Medical School, in the plenary address at IHI's 11th Annual National Forum on Quality Improvement in Healthcare.
Online patients
At what point in the health care process do patients typically seek out health care information via the World Wide Web?

Source: Cyber Dialogue, June 2000.
HCFA finds overpricing of Rx drugs
The Health Care Financing Administration (HCFA) is encouraging Medicare claims processors to reduce reimbursements for prescription drugs, according to the June 2 Washington Post.
The lower reimbursement rates are a result of an ongoing federal investigation which revealed that Medicare and Medicaid have been overpaying for prescription drugs because of suspect pricing practices by pharmaceutical companies. Investigators say that average wholesale prescription prices, which are what Medicare and Medicaid base their payments on, are inflated by pharmaceutical companies, which then sell the drugs to physicians and pharmacies at large discounts. The Health and Human Services' Office of Inspector General estimates that Medicare pays from 11 percent to 900 percent more for drugs than physicians do.
