
With tremendous change taking place in health care, the mood among family physicians is anxious, but there are reasons to be hopeful.
Fam Pract Manag. 2017;24(1):26-33
Author disclosures: no relevant financial affiliations disclosed.

Almost 50 years ago, in 1969, family medicine was officially recognized as a medical specialty in the United States. In many ways, the past five decades could be described as an uphill climb as the new specialty fought for respect and proved its value by delivering higher quality care for a lower price.1
Today, amid massive shifts in payment and care delivery models, how are family physicians faring? This article explores that question, drawing on data from the American Academy of Family Physicians (AAFP) and other sources, and examines what lies ahead for the specialty.
The good news
We begin with one of the most basic measures of success – money. In recent years, family physicians have seen modest gains in real income. The mean for all family physicians in 2014, the most recent AAFP data available, was $195,310; the median was $185,000 – a 15.6 percent increase from five years earlier. (See “Distribution of family physicians by annual income.”) Meanwhile, the income gap between primary care and non-primary-care physicians has decreased from 44.6 percent in 2011 to 41 percent in 2015, according to AAFP data.
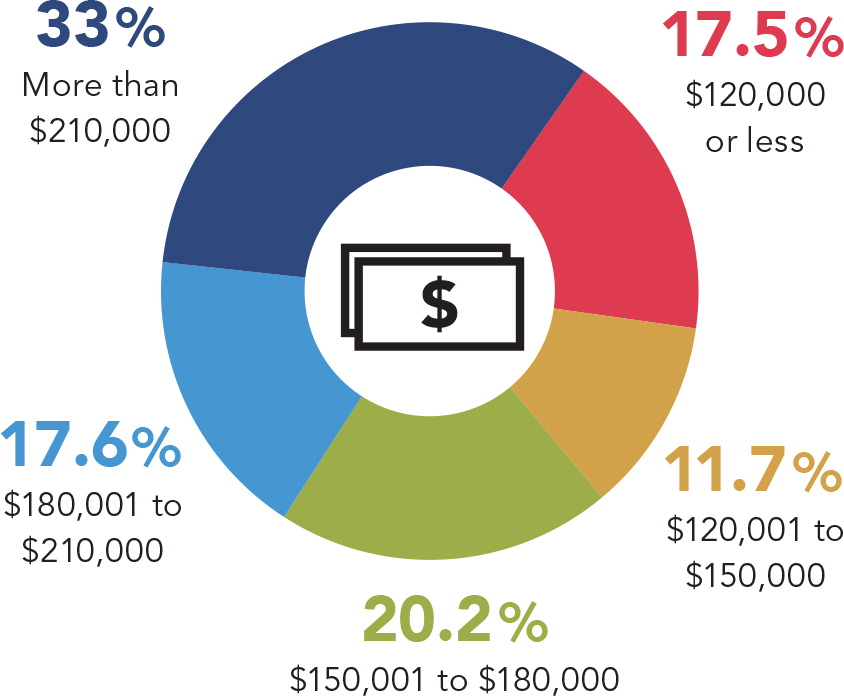
Median income for all family physicians increased to $185,000 in 2014, although it varied widely; the mean was $195,310. Incomes averaged $180,000 for employed physicians and $200,000 for owners. Five years earlier, the median income for all family physicians was $160,000, the equivalent of $176,556 in 2014 dollars.
Source: AAFP. 2015 Practice Profile. July 2016.
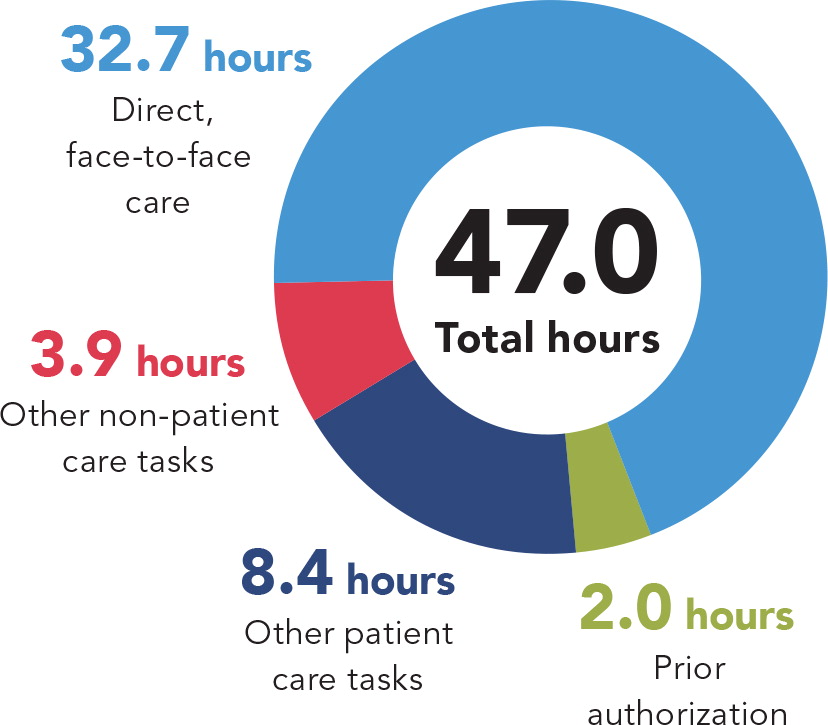
On average, family physicians spend 47 hours per week in practice with nearly 33 hours spent in direct, face-to-face patient care. These numbers are down slightly from five years ago.
Source: AAFP. 2015 Practice Profile. July 2016.
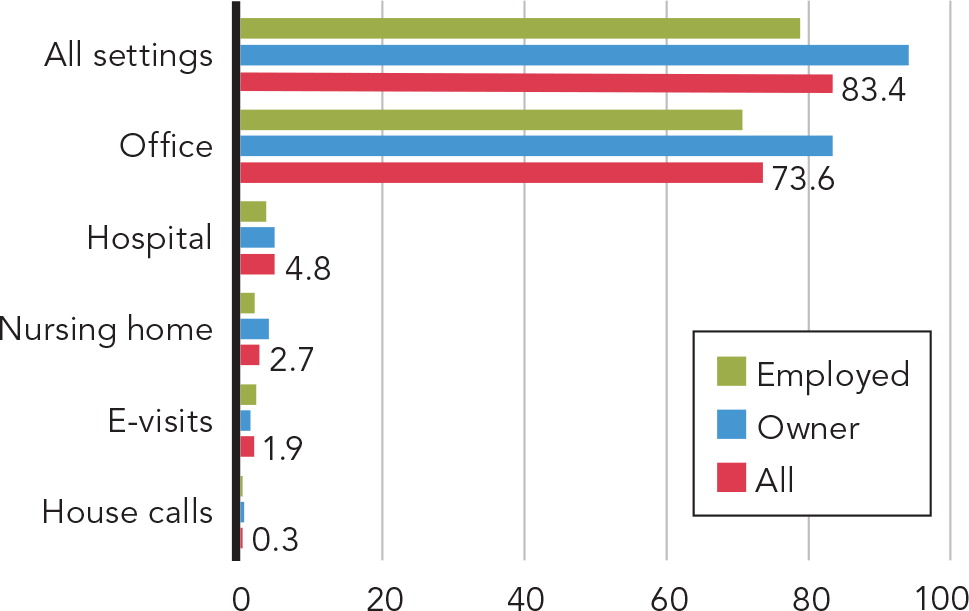
On average, family physicians see 83 patients per week in all settings. This number has been decreasing since 2010, when it averaged 99 patients per week.
Source: AAFP. 2015 Practice Profile. July 2016.
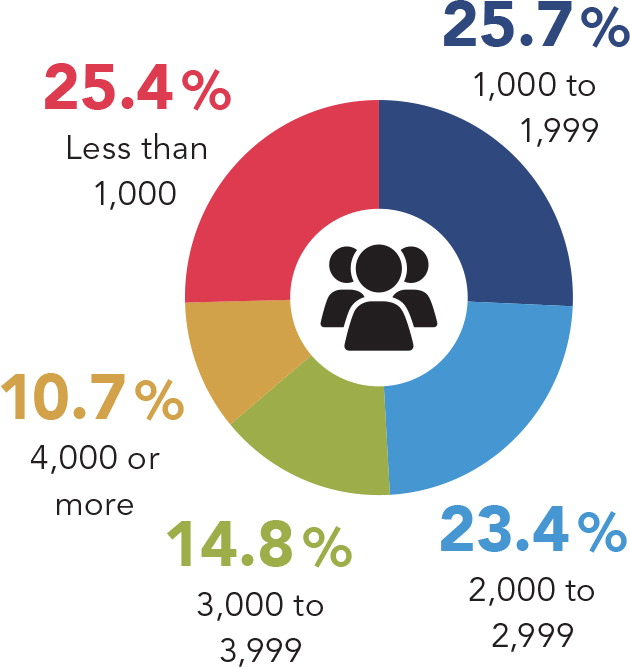
The average patient panel size among family physicians surveyed was 2,194 patients. The median was 2,000. Panel size was defined as “the number of patients attributed to you and seen in the past 24 months.”
Source: AAFP. 2015 Practice Profile. July 2016.
Physician search firm Merritt Hawkins & Associates reports that family physicians are “at the top of the wish list for hospital and medical group administrators,”2 which is helping to strengthen salaries and signals high demand.
“The value of primary care – the efficiency and quality that we bring to the system – is becoming more widely recognized,” said AAFP president-elect John Meigs Jr., MD, FAAFP, of Centreville, Ala. “And we are beginning to get paid for it.”
For example, the Medicare Primary Care Incentive Payment Program, which was mandated as part of the Affordable Care Act (ACA), has provided a 10 percent quarterly bonus to most primary care physicians since 2011, although it recently expired. Many payers have developed similar programs to reward effective primary care, and the Medicare Access and CHIP Reauthorization Act (MACRA) promises improved payment for those who can prove their value.
Payment is “still not where it ought to be,” said Meigs, “but I think we are beginning to see some respect for the value that we bring to the system.”
First-contact, person-focused, comprehensive, coordinated care – the hallmark of family medicine – is becoming even more important as the health system transitions to value-based payment. “Primary care physicians are best positioned to coordinate care and drive savings in a value-based health care system, and there's real demand for a model that cements primary care as its foundation,” said Farzad Mostashari, MD, former National Coordinator for Health IT and now chief executive officer of Aledade, which partners with primary care physicians to build and lead accountable care organizations.
He said he believes that primary care practices can “reassume their role at the center of patient care by taking responsibility for a patient's overall health and health spending.” This bodes well for primary care physicians in all settings if they are willing to embrace this role, but it should be especially encouraging for those who have remained in independent practice, said Mostashari. “In this system, independent primary care doctors are particularly well-suited as they do not have the pressures of a larger health system and are free to adopt the partners and tools needed to thrive,” he said.
Continued recognition of the value of primary care, and continued increases in income, will play a vital role in family medicine's ability to grow and to attract more medical students. For the last seven years, the number of students matching with family medicine residency programs has increased steadily, after roughly a decade of decline. (See “Number of students matching with family medicine.”)
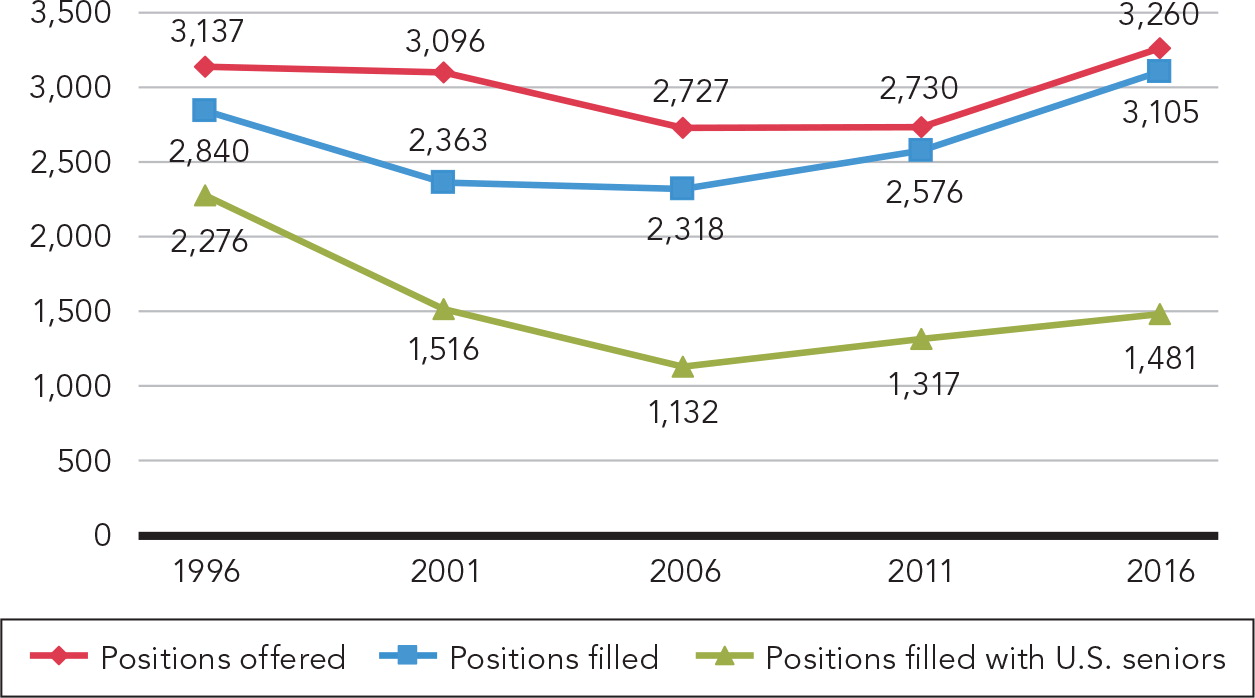
In 2016, for the seventh straight year, the family medicine match rate increased. Of the 3,105 positions filled, 1,481 were filled with seniors of U.S. allopathic medical schools. The remaining positions were filled with U.S. citizen graduates of international medical schools (729), graduates of osteopathic medical schools (385), non-U.S. citizen graduates of international medical schools (382), previous graduates of U.S. allopathic medical schools (127), and graduates of Canadian medical schools (1).
Source: National Resident Matching Program.
Although the number of students selecting family medicine or another primary care specialty is not yet high enough to solve the primary care shortage, Meigs is optimistic. “If we continue along the way of improved payment, recognition of the value we bring to the system, and increased respect by our peers and the system, then I think you will begin to see our numbers ticking up more.”
Now, the not-so-good news
Despite increases in income, demand, and match rates, an alarming 63 percent of family physicians meet the criteria for burnout, compared with 54.4 percent of all physicians. When asked how they feel about the current state of the medical profession, 50.5 percent of primary care physicians report positive feelings. For comparison, just 43.5 percent of specialists report positive feelings about the current state. (See “Physician burnout rates” and “Primary care physicians' attitudes toward the medical profession.”)
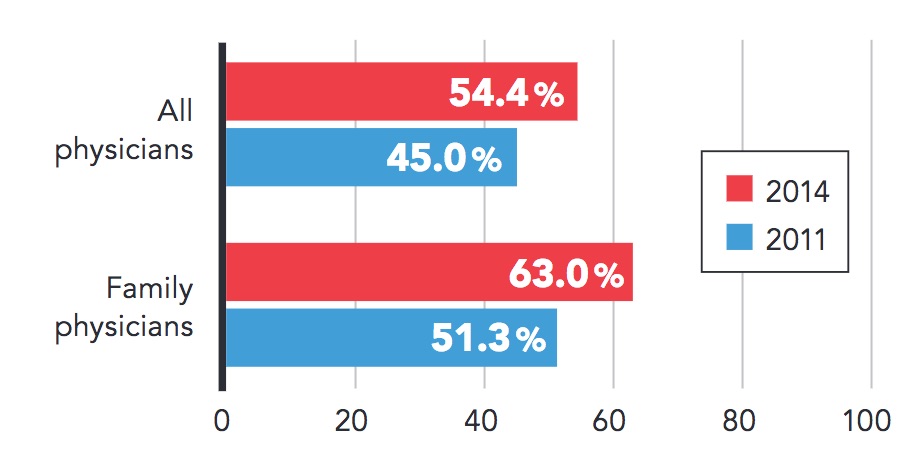
An estimated 63 percent of family physicians met the criteria for burnout in 2014, an increase from three years earlier. The burnout rate among family physicians is higher than the rate among all physicians.
Source: Shanafelt TD, Hasan O, Dyrbye LN, et al. Changes in burnout and satisfaction with work-life balance in physicians and the general U.S. working population between 2011 and 2014. Mayo Clin Proc. 2015;90(12):1600–1613.
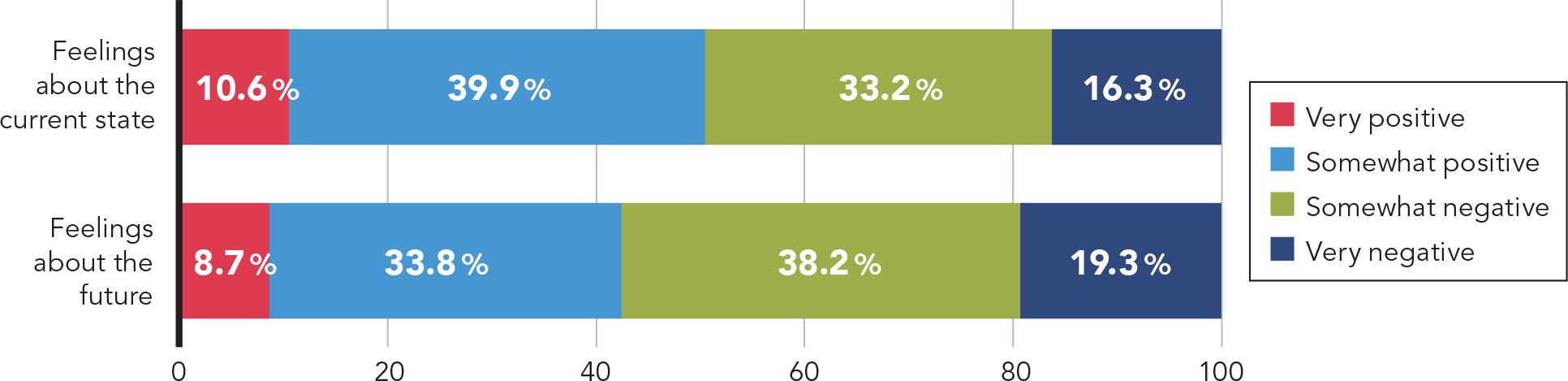
While 50.5 percent of primary care physicians report positive feelings about the current state of medical practice, 42.5 percent report positive feelings about the future of the medical profession. These percentages are higher than those reported by specialists – 43.5 percent and 33.9 percent, respectively.
Source: The Physicians Foundation. 2016 Survey of America's Physicians. September 2016.
“There's a growing sense, which we've seen since 2012, that physicians just feel overwhelmed, overtaxed, and are now looking for their own self-preservation,” said Ripley Hollister, MD, FAAFP, a Colorado Springs, Colo., family physician and board member of the Physicians Foundation. “The patient interaction and the intellectual challenge of practicing medicine are the two main reasons doctors are in medicine. But because of all of the administrative hassles and the various requirements of health care reform and quality metrics, physicians are becoming more and more inundated with things that separate them from the one thing that they love, which is patient care.”
A recent study estimated that for every one hour physicians spend in patient care, they spend two hours on administrative work – mostly electronic health record (EHR) and desk work.3 Informing federal agencies and large health systems of this reality could be the first step toward alleviating this burden.
“We must reduce the administrative hassle of modern medical practice,” said Meigs, pointing to its effects on physician productivity and morale. “I think I am a better physician now than I was 10 years ago. I have that much more years of experience and I know my patients that much better, but I can't see as many patients as I did 10 years ago. It's not because I'm slow. It's just all the other junk I have to do. That is frustrating.”
Another major frustration is the economics of running a medical practice. It used to be that physician practices “could actually anticipate a stable budget as long as the covered lives remained consistent,” said Karen L. Smith, MD, FAAFP, a solo family physician in Raeford, N.C, and the AAFP's 2017 Family Physician of the Year. But a stable budget is no longer the norm. The inability to negotiate fair rates with insurance companies and fair prices with vendors “has always been and continues to be an issue,” she said. And with large numbers of uninsured or underinsured patients and a rising number of self-pay patients, “the practice absorbs much of the unpaid services provided despite maximal collection effort,” said Smith.
To escape the growing financial and administrative challenges, increasing numbers of physicians have been leaving independent practice and moving to employed settings. Two-thirds of family physicians now say they have no ownership stake in their practices, and hospitals or health systems are the most common employer, although most family physicians still practice in small group settings averaging 6.6 physicians. (See “Distribution of family physicians by practice ownership.”)
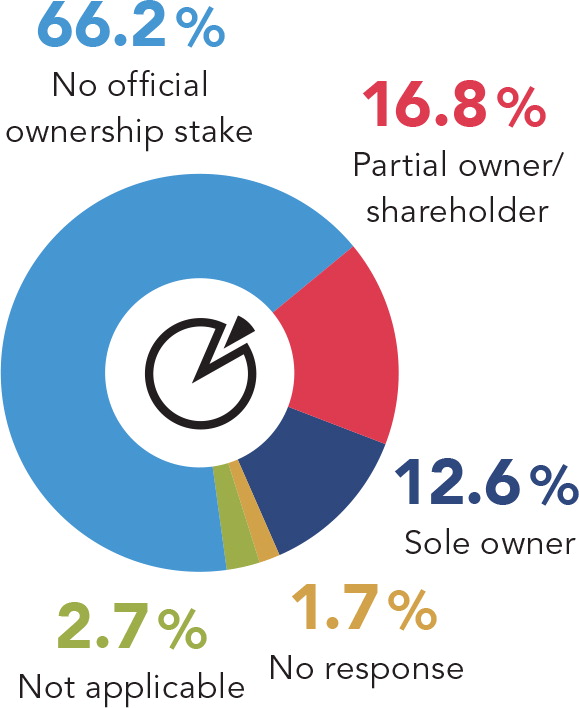
Two-thirds of family physicians have no ownership stake in their practices, while 29 percent have sole or partial ownership.
Source: AAFP Member Census. Dec. 31, 2015.
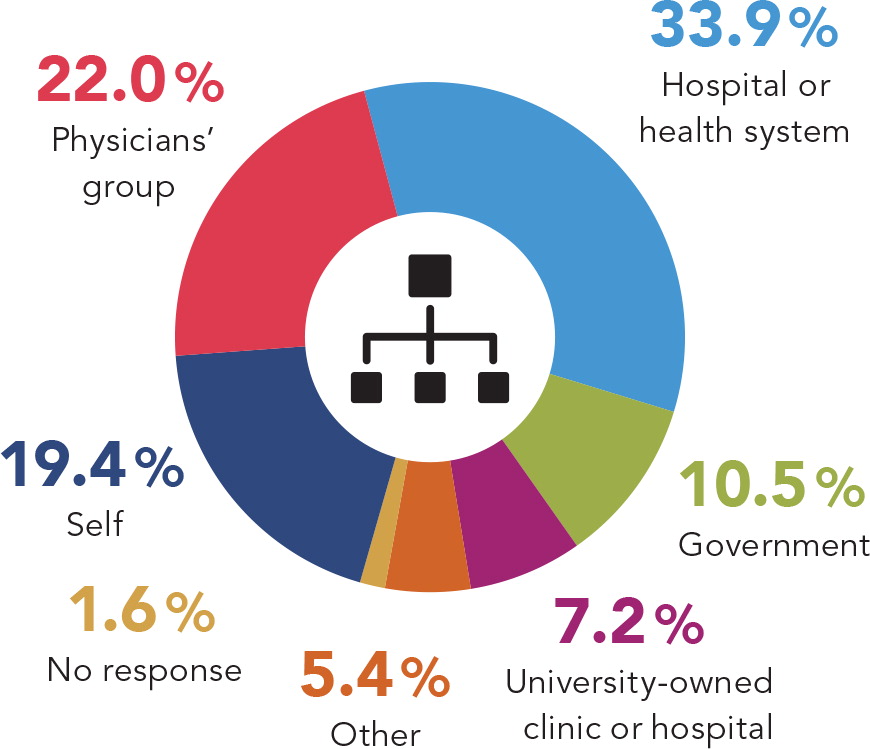
Thirty-four percent of family physicians consider their primary employer to be a hospital or health system, followed by 22 percent whose primary employer is a physicians' group. Nineteen percent consider themselves to be their primary employer (self-employed, majority practice owner, independent contractor, etc.). Compared with data from five years earlier, the hospital/health system segment has grown 4 percentage points while the self-employed segment has decreased 5 percentage points.
Source: AAFP Member Census. Dec. 31, 2015.

Although more family physicians are moving into employed settings, the average practice size remains fairly small – a mean of 6.6 full-time-equivalent physicians, or a median of just 3.0. Practices average 17.5 support staff, or 2.7 per physician.
Source: AAFP. 2015 Practice Profile. July 2016.
However, for some, employed practice may not be the remedy they hoped it would be. “The inability to express creativity and thought toward the business management of the practice as part of a larger group may be a stress reliever for some,” said Smith, “but others may find the environment to be of such restriction as to stifle optimal performance.”
Hollister notes that even employed physicians have had to become “more managerial,” but in a new way – managing a patient population and a care team, for example. Adapting to this new role can be frustrating, but Hollister believes it is essential. “I think primary care is coming into its own as we recognize the importance of having someone managing all of the factors around patient care and optimizing them for quality and value,” he said.
For now, though, many family physicians feel that they are “straddling two worlds, and it's giving people heartburn,” said Meigs. It's the old world of predominantly paper-based, independent, fee-for-service practice versus the new world of increased consolidation, increased technology, and value-based care. “Anytime you're going through a major change, that brings anxiety and uncertainty,” said Meigs. “We have to survive in the old system as we transform our practices to the new system, so we have to function in two worlds and do it in such a way that we remain financially viable and take care of our patients.”
If it's any consolation, Hollister notes that primary care physicians are slightly more positive about medical practice than other specialists, according to data from the Physicians Foundation. He speculates that the patient relationship makes all the difference. “If you're a specialist, you encounter a patient population of 10,000 to 15,000, much different from primary care where we have 3,000 to 4,000 patients. We excel at the physician-patient relationship, and we are better able to hold on to that in times of great change.”

Just under half of family physician respondents said their practice has been designated as a patient-centered medical home. This is a significant increase over previous years; in 2013, just 26 percent said their practice had been designated as a patient-centered medical home.
Source: AAFP. 2015 Practice Profile. July 2016.
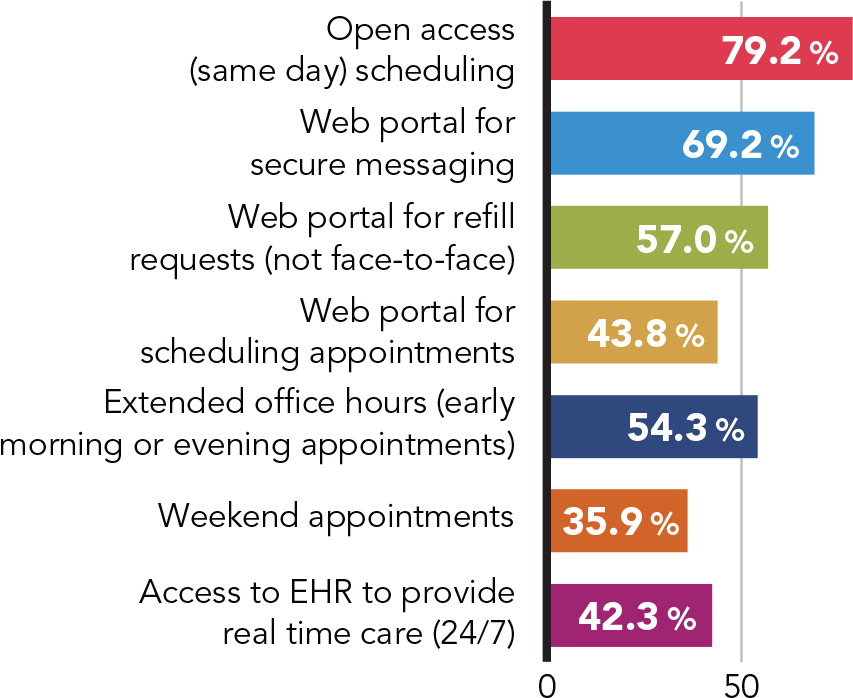
Family physicians use a variety of strategies to improve patient access, with the most common being open-access scheduling (79 percent) and a web portal for secure messaging (69 percent).
Source: AAFP. 2015 Practice Profile. July 2016.
What lies ahead
With the current trend toward consolidation and employed practice, one might think that the future of family medicine has no place for small independent practices. Not so, said Mostashari. “There is no evidence that consolidation of hospitals and physician practices leads to better clinical outcomes or cost reductions. In fact, recent studies4 suggest that small, physician-owned practices have a lower average cost per patient, fewer preventable hospital admissions and lower readmission rates than hospital-owned practices,” he said.
“We need small practices to survive. Many doctors want to practice this way. Many patients want the real relationship that comes with seeing a solo provider. And as the evidence shows, the health care system needs these independent voices to boost outcomes and help bring down costs,” Mostashari said. “My hope and belief is that policy-makers and payers will understand that keeping independent small practices afloat is good for society and good for patients. Making it easier for practices to come together and share the costs of quality reporting, supporting advanced payment models that do not subject small practices to crippling risk, and creating a level playing field between hospital and clinic payments are all actions that can help, and I hope that we will see taken.”
With the recent presidential election and talk of repealing and replacing the ACA, health care is “full of uncertainty,” Meigs said. Physicians will have to see if inroads made under the Obama administration regarding the importance of primary care will continue under the Trump administration. But there are no signs that the shift to value-based care and payment will slow down in the near future. MACRA, which was passed with bipartisan support in Congress, is separate legislation from the ACA, and physicians will need to begin reporting quality and cost measures in 2017 under the Merit-Based Incentive Payment System (MIPS) to avoid a payment penalty beginning in 2019. Alternatively, physicians can form or join an advanced alternative payment model. (See the article “Making Sense of MACRA, Part 2: Value-Based Payment and Your Future.”)
Meigs acknowledges that these provisions will pose challenges for family physicians as they attempt to understand and comply with a new set of lengthy and complex regulations. But he notes that family physicians are ahead of many other specialists when it comes to managing costs and reporting on quality.
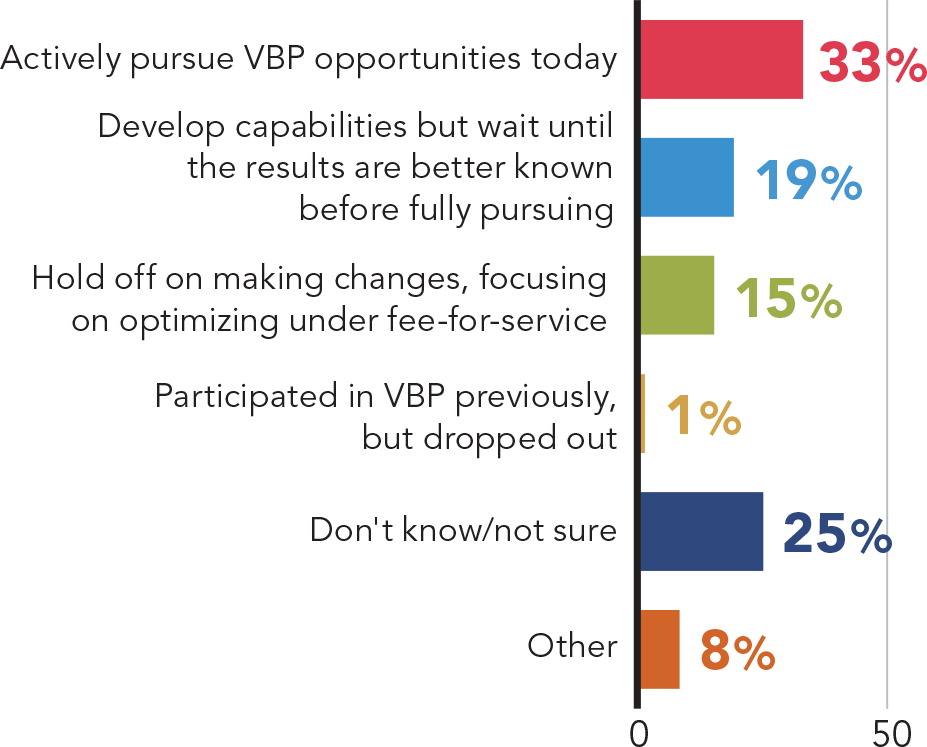
When asked about their involvement in value-based payment, about half of family physician respondents said they are either actively pursuing value-based payment or developing capabilities.
Source: AAFP. Value Based Payment Survey. October 2015.
To succeed in value-based care, said Mostashari, practices will need to ingrain it into their culture and continually refocus on why they are doing the work – for patients. “Taking a patient-centered approach allows the focus to shift from one of compliance to a focus on outcomes and allows for more day-to-day meaning and motivation,” he said. “If primary care physicians truly believe that preventing one hospital admission for a vulnerable patient creates as much value for the practice as seeing 50 routine office visits, then they will succeed in reducing admissions. If, on the other hand, they continue to see their practice through the ‘fee-for-service’ lens, they may not see the returns they hope from new payment models.”
However, even if primary care physicians see improved payment, that doesn't erase the fact that MACRA will be “one of the most aggressive changes encountered in a long time,” said Smith. “The projected bonuses for MACRA do not make up for the years of lost revenue already encountered and the cost of implementation of workflow modification and technology.”
It's possible that the challenges of value-based payment may be too much for some physicians. “Some family physicians may find it necessary to drop off the bandwagon of traditional care delivery and strongly consider other options that will suit both the doctor and the patients served,” said Smith, alluding to alternative practice options such as direct primary care. Currently, just three percent of family physicians are in a direct primary care practice, according to AAFP data, but the model is spreading.
Hollister believes that with time, as family physicians adjust, frustrations will lessen and satisfaction will rise. Family physicians have a long history of adapting to change, and the new generation of physicians appears to have more optimism.
“I think it's because they graduated from residency with a different set of skills,” Hollister said. “They've been engaged in quality metrics in medical school. They've been engaged with EHRs.” As a result, newer physicians may be coping better, he said.
For veteran physicians who feel beaten down by the tremendous changes that have taken place in health care over the last decade, Smith said it is important to remember that “our self-worth remains within our control.”
She suggests taking some time for self-reflection: “This is a time to take a break from the practice treadmill, plan a personal retreat for a day or weekend as needed, and think about where you are in your professional career and where you want to be in five and then 10 years, recognizing MACRA full implementation will not be realized until the year 2024.” Consider personal and family needs, changing patient demographics, physical and technology expansion or updates, and potential partners or competitors, she said. “Add any other factors as deemed necessary to allow a sketch of your physical, mental, and emotional strategy for continued practice as a family physician.”
Most important, said Smith, remember that “Success is determined by how you define it.”
Approaching the summit
Five years ago,5 Family Practice Management reported on the state of family medicine and concluded, “It is at once incredibly challenging and incredibly rewarding” – a tension that still holds true today.
“Most family physicians are taking care of their patients every day while also trying to stay afloat as a business,” said Mostashari. “They derive great satisfaction and meaning from their work, but face a complicated health care system where their role as quarterback for their patients' care is not always respected, where regulations and ‘administrivia’ keep piling on, and they worry about the impact on their patients and practices of the ever-changing payment models and policies – change that only seems to be accelerating. Many are fearful and discouraged, some are overwhelmed.”
At the same time, family physicians should be encouraged by increased demand for their services, increased income, and the promise of value-based payment models that could put primary care physicians “back in the center and in greater control, with the opportunity for big returns if they can do the right things for their patients and keep them healthy and out of the hospital,” said Mostashari. “In sum, the mood is anxious for many, but hopeful for those who have found the right partners to help them navigate these changes.”
Almost 50 years after the start of its journey, is it possible that family medicine is nearing the summit, or will the uphill climb continue? It may be too early to tell. But either way, family medicine has a lot to be proud of. You've come a long way.
