
Am Fam Physician. 2024;109(1):online
Author disclosure: Dr. Harper's institution received a research grant from Roche for her work on an economic analysis of dual staining cytology as a triage test for patients testing positive for high-risk HPV subtypes. Drs. Bettcher and Young have no relevant financial relationships.
Cervical cancer screening aims to detect cervical intraepithelial neoplasia grade 3 or higher (CIN 3+) to reduce morbidity and mortality from cervical cancer.1 This strategy has evolved from vaginal to cervical specimens in the 1960s, from cytology alone to cytology with human papillomavirus (HPV) triage in the 1990s, and from cotesting using both cytology and HPV testing in the 2010s to, most recently, primary HPV testing. Primary HPV testing is an effective screening modality for cervical cancer in average-risk individuals (eTable A), can decrease the total number of screenings a patient needs, and can decrease inequities in cervical cancer screening and follow-up testing.
| Population | Recommendation |
|---|---|
| Low risk Patients who have had a hysterectomy (including the cervix) because of benign conditions Patients with a cervix but who have comorbidities and decreased life expectancy | No testing |
| Average risk Patients 25 to 65 years of age with a cervix | Primary HPV testing |
| High risk* Patients 30 to 65 years of age with a cervix and a high-risk condition (i.e., solid organ transplantation, chronic diseases managed by Janus kinase inhibitors or biologics, immunosuppressive drug treatment, HIV/AIDS, postcoital bleeding, or under surveillance for prior HPV-positive testing per American Society for Colposcopy and Cervical Pathology guidelines) | Cotesting |
The U.S. Preventive Services Task Force and the World Health Organization recommend primary HPV screening as an option (some as preferred) for cervical cancer screening.2–6 Primary HPV screening has been thoroughly tested in 13 population-based randomized controlled trials over 15 years of follow-up.7–14 All trials found that primary HPV screening is as effective at detecting incident CIN 3+ as cotesting, with fewer harms.
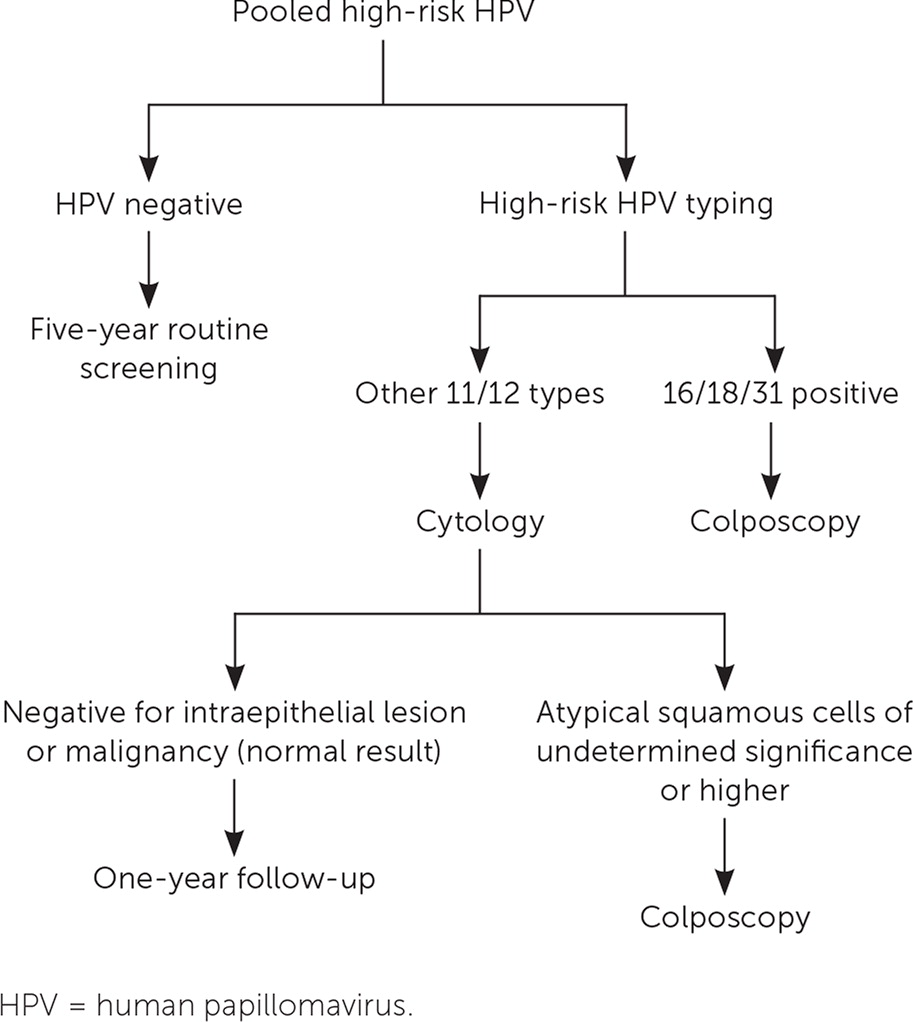
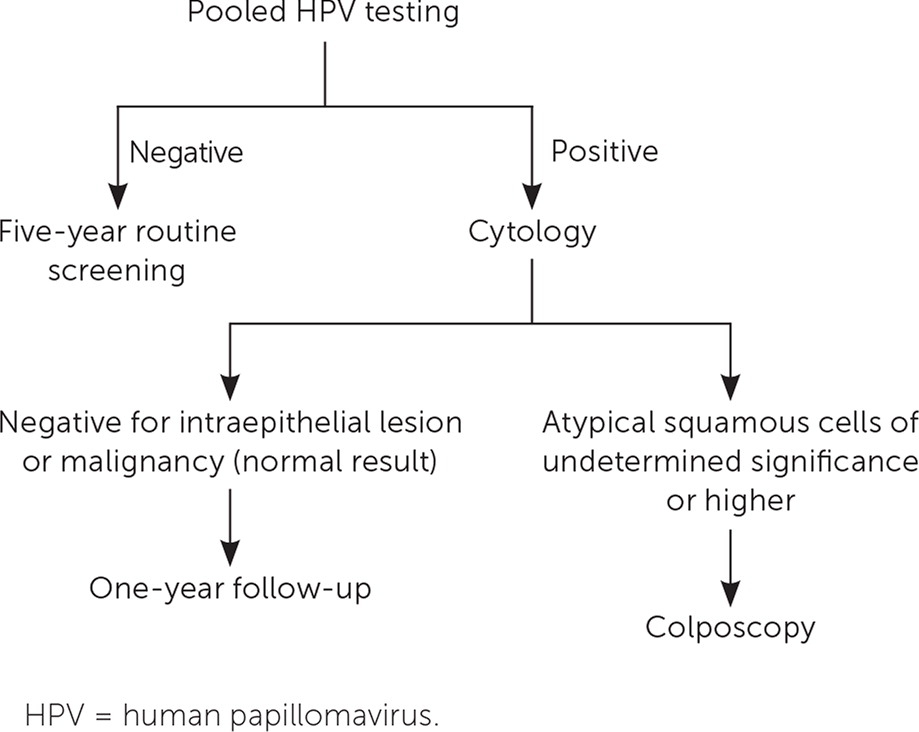
With primary HPV testing, patients experience the same speculum examination as they do with cotesting; the difference is what happens in the laboratory and with the result. The primary HPV screening tests approved by the U.S. Food and Drug Administration (FDA) are the Roche Cobas and BD Onclarity tests (eTable B). HPV results for the Roche and BD tests can be reported as a pooled result. This means the physician receives a result of negative or positive, in which positive indicates that at least one, but possibly more, types of high-risk HPV were identified in the sample. HPV genotyping options differ by manufacturer. Roche Cobas reports HPV 16 and 18 individually and groups 12 other types (i.e., positivity means at least one of the 12 types triggered the positive result). BD Onclarity reports six individual HPV types (16, 18, 31 [the highest risk going immediately to colposcopy], 45, 51, and 52), and three groups of combined types (33/58), (35/39/68), and (56/59/66). Figure 1 and Figure 215 describe management strategies following a negative or positive primary HPV screening result with or without genotyping.
| Indication* | Test name | Manufacturer | Results |
|---|---|---|---|
| Primary HPV testing | Cobas HPV | Roche | Pooled 14 high-risk HPV: positive/negative Genotype specific: 16, 18, and type group (31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68) |
| Primary HPV testing | BD HPV Onclarity | BD | Pooled 14 high-risk HPV: positive/negative Genotype specific: 16, 18, 31, 45, 51, 52, and type groups (33/58), (35/39/68), (56/59/66) |
| Triage after ASCUS cytology or cotesting with cytology | Cervista HPV HR | Hologic Gen-Probe | Positive, negative, indeterminate |
| Triage after ASCUS cytology or cotesting with cytology where the Cervista HPV HR test was used as the triage test | Cervista HPV 16/18 | Hologic Gen-Probe | Positive for genotype, negative, indeterminate |
| Triage after ASCUS cytology | Aptima HPV | Hologic Gen-Probe | Positive, negative, invalid |
| Triage after ASCUS cytology or cotesting with cytology where the Aptima HPV HR test was used as the triage test | Aptima HPV 16 18/45 | Hologic Gen-Probe | Positive for genotype, negative, invalid |
| Reflex triage after ASCUS cytology | Digene Hybrid Capture 2 HPV DNA | Qiagen | Positive/negative |
Although primary HPV screening is as effective as cotesting at detecting cervical cancer, primary HPV screening decreases the number of lifetime screenings needed. The U.S. Preventive Services Task Force has modeled different screening strategies, defining harms as the lifetime number of tests, colposcopies, false-positive results, cervical cancer cases, and cervical cancer deaths.6 Benefits were defined as life-years gained, disease detected, and cancer averted. Modeling the screening strategy of cervical cytology alone every three years for women 21 to 29 years of age, followed by cotesting every five years for women 30 to 65 years of age, led to the highest number of lifetime cytology tests per 1,000 women (eTable C). For the individual, primary HPV screening provides equally accurate disease detection with fewer tests.
| Strategy | Cytology tests | HPV tests | Total tests* | Colposcopies | Total tests/CIN3+ | Colposcopies/CIN3+ | Total workup/CIN3+ |
|---|---|---|---|---|---|---|---|
| Cyto-3y,21/COTEST-5y,30 | 11,425 | 8,380 | 19,806 | 1,630 | 366.8 | 30.2 | 397 |
| Cyto-3y,21/HPV-5y(16/18),30 | 3,675 | 8,476 | 12,151 | 1,635 | 229.3 | 30.8 | 260 |
| Cyto-3y,21/HPV-5y(cyto),30 | 3,888 | 8,459 | 12,348 | 1,452 | 233.0 | 27.4 | 260 |
Primary HPV screening is currently performed with a speculum examination; however, in the near future, it will be FDA-approved for vaginal self-sampling.16 Self-sampling is reasonable because HPV is transmitted skin-to-skin and must travel through the vagina before reaching the cervix. Two self-sampling approaches have been found to be effective. The vaginal approach uses a device similar to a thin tampon that the patient inserts into the vagina, turns several times, places in a transport tube (some with liquid media), and returns. The urine approach is similar to collection for sexually transmitted infection testing by gathering the desquamated cells coming from the cervix, vagina, and external genitalia in the first part of the urine stream. Both techniques are noninferior to clinician sampling at the os.17,18 Self-sampling promotes health equity by allowing more women to obtain their own sample, potentially increasing the number of women who complete screening. Early cost-effectiveness analyses suggest overall cost savings but, more importantly, that the savings from not performing cotesting could cover current out-of-pocket costs for colposcopy. The Affordable Care Act mandates coverage only for screening tests. However, should the U.S. Congress amend it to cover all screening and evaluation costs for cervical cancer, payors could easily shift the costs from unnecessary cytology screening to cover the out-of-pocket costs for colposcopy, as they have done for colorectal cancer screening.
Primary HPV screening benefits patients by limiting unnecessary testing, benefits physicians by providing a simpler strategy for management, and benefits society by making cervical cancer screening more accessible. Now is the right time for family physicians to shift our cervical cancer screening strategy from cotesting to primary HPV screening for average-risk, asymptomatic women.
