
Am Fam Physician. 1998;57(5):946-947
to the editor: We describe here a case of mediastinal germ cell tumor in a patient with human immunodeficiency virus (HIV) infection. A 30-year-old man presented with a three-day history of dyspnea, cough and fever. He had had pneumonia six months prior. He used cocaine, tobacco and, occasionally, alcohol. Physical examination revealed the following findings: mild dyspnea; pulse, 110 per minute; blood pressure, 120/70 mm Hg; temperature, 38.3°C (101°F); respiration 20 per minute, with crepitations at the lung bases. The remaining physical examination was unremarkable.
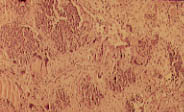
Laboratory evaluation showed a total white blood cell count of 12,400 per mm3 (12.4 × 109 per L), with 74 percent (0.74) neutrophils, 12 percent (0.12) bands, 9 percent (0.09) lymphocytes, 4 percent (0.04) monocytes and 1 percent (0.01) basophils. Lactate dehydrogenase was 472 U per L. Chest radiographs and computed tomography (CT) scan of the chest showed a large anterior mediastinal mass and bilateral interstitial infiltrates. CT scan of the abdomen and pelvis did not reveal lymphadenopathy or mass. A limited anterior thoracotomy showed a 10 to 15 cm soft and rubbery mass in the anterior mediastinum. Biopsy of the mass confirmed the diagnosis of malignant germ cell tumor (see figure) comprising a combination of seminomatous and nonseminomatous elements in the form of embryonal carcinoma and choriocarcinoma.
Further laboratory investigations revealed positive HIV1 antibodies with an absolute CD4+ cell count of 110 cells per mm3 (200 × 106 per L). Alpha-fetoprotein was normal (5.5 ng per mL [5.5 μg per L]) but the human chorionic gonadotropin (hCG) level was very high (90,100 mIU per mL [90,000 IU per L]). Ultrasonogram of both testicles was normal.
The patient was offered chemotherapy and radiotherapy but elected to receive therapy at an institution closer to his home.
Primary mediastinal germ cell tumors are rare and not often reported in patients infected with HIV.1 Patients may remain asymptomatic or may present with cough, dyspnea and chest pain.2 Histologically, germ cell tumors are classified as seminomas or nonseminomas. Nonseminomas are further subclassified as embryonal cell tumors, choriocarcinomas or teratomas. Seminomas are radiosensitive, while nonseminomas are radioresistant. Alpha-fetoprotein and hCG are useful tumor markers. Serum alpha-fetoprotein is elevated in 85 percent of patients with nonseminomatous tumors. Pure seminomas do not produce it. Generally speaking, alpha-fetoprotein is produced by embryonal cell carcinoma and hCG by choriocarcinoma. A high lactate dehydrogenase level is also considered an independent prognostic predictor.
Treatment consists of surgery, radiotherapy and cisplatin-based combination chemotherapy. Mediastinal nonseminomas carry a poor prognosis. Approximately 50 percent of patients survive after cisplatin-based chemotherapy followed by aggressive resection. Mediastinal seminomas, on the other hand, have a five-year disease-free survival rate of over 80 percent.3