
Am Fam Physician. 1998;57(9):2135-2142
A more recent article on slipped capital femoral epiphysis is available.
See related patient information handout on slipped capital femoral epiphysis, provided by an AAFP staff patient education writer.
Slipped capital femoral epiphysis occurs during the adolescent growth spurt and is most frequent in obese children. Up to 40 percent of cases are bilateral. Recent classification methods emphasize epiphyseal stability rather than symptom duration. Most cases of slipped capital femoral epiphyses are stable and have a good prognosis if diagnosed early. Unstable slipped capital femoral epiphysis has a much poorer prognosis because of the high risk of avascular necrosis. Early radiographic clues are the metaphyseal blanch sign and Klein's line. Once diagnosed, treatment should begin immediately. The most widely accepted treatment for a stable slipped capital femoral epiphysis is in situ fixation with a single central screw. The treatment for an unstable slipped capital femoral epiphysis is much more controversial. Corrective osteotomy is usually reserved for treatment of severe deformities after the patient has stopped growing.
Slipped capital femoral epiphysis is defined as a posterior and inferior slippage of the proximal femoral epiphysis on the metaphysis (femoral neck), occurring through the physeal plate during the early adolescent growth spurt. It is the most common hip disorder in adolescents, but because of the anatomic innervation of the hip and the referred nature of the pain, it often presents with groin, thigh or knee pain rather than hip pain. Thus, diagnosis is often enigmatic and, unfortunately, in many instances, it is initially missed, which delays treatment. This delay results in a less favorable long-term prognosis. The diagnosis of slipped capital femoral epiphysis should always be considered when a physician is assessing the causes of limp and/or hip, thigh and knee pain in children (Table 1).
| Disorder | Typical age of onset (years) | Gender ratio (m:f) | Typical percentage of bilaterality |
|---|---|---|---|
| Developmental hip dislocation | 0 to 2 | 1:4 | 20 |
| Legg-Calvé-Perthes disease (aseptic necrosis of the femoral head) | 4 to 8 | 5:1 | 10 |
| Slipped capital femoral epiphysis | 10 to 15 | 1.5:1 | 25 to 40 |
Classification
The traditional classification for slipped capital femoral epiphysis is based on duration of symptoms.1,2 Patients with symptoms of less than three weeks' duration are classified as acute; patients with symptoms lasting for three weeks or more are considered chronic, and those with symptoms of more than three weeks' duration but with a recent, sudden exacerbation of symptoms are classified as acute-on-chronic. This classification system may be difficult to use because the duration of symptoms is often vague, making it impossible to accurately classify the slipped capital femoral epiphysis; in addition, this classification is not prognostic with regard to long-term outcome and the most serious complication, avascular necrosis.
More recently, slipped capital femoral epiphysis has been classified according to stability2; a stable slipped capital femoral epiphysis is one in which ambulation is possible, with or without crutches, and an unstable slipped capital femoral epiphysis is one in which ambulation is not possible, with or without crutches. The unstable slipped capital femoral epiphysis behaves much more like an acute fracture and has a poorer prognosis because it carries an increased risk of avascular necrosis. In most cases, slipped capital femoral epiphyses are stable and typically account for at least 90 percent of all cases.
Etiology
Although slipped capital femoral epiphysis can be associated with endocrine disorders (e.g., hypothyroidism or growth hormone administration), renal osteodystrophy and radiation therapy, most cases are idiopathic in nature. This article focuses only on idiopathic slipped capital femoral epiphysis.
Idiopathic slipped capital femoral epiphysis may be caused by many factors, including obesity, physeal orientation, abnormalities in physeal architecture and hormonal changes during adolescence that affect physeal strength. Obesity results in increased sheer stress across the physeal plate, which is already oriented more vertically and posteriorly (retroversion) in children with slipped capital femoral epiphyses. This stress, combined with a weaker physeal plate related to architectural irregularities and endocrine changes associated with puberty, leads to slippage of the epiphysis inferiorly and posteriorly in the direction of the weight-bearing force.
Demographics and Physical Characteristics
Although slipped capital femoral epiphysis is usually associated with obesity (defined as above the 95th percentile of weight for age), it can also occur in children who are not obese.3 Children of all races can have a slipped capital femoral epiphysis; however, it is probably more common in black or Polynesian children and occurs slightly more often in boys than in girls (60 percent versus 40 percent). Slipped capital femoral epiphysis occurs during the pre-pubescent growth phase and almost never occurs in girls once menses have begun. In a large series of children with slipped capital femoral epiphysis,3 the average age and standard deviation was 12.0 years (±1.5 years) in girls and 13.5 years (±1.7 years) in boys. Slipped capital femoral epiphysis is bilateral in 25 to 40 percent of children.4 One half of children with bilateral involvement present with simultaneous slipped capital femoral epiphyses; the other one half present with a unilateral slipped capital femoral epiphysis and later develop the condition in the opposite hip, usually within 18 months of the first presentation.
History and Physical Examination
Stable Slipped Capital Femoral Epiphysis
Typically, a child with a stable slipped capital femoral epiphysis has a history of intermittent limp and pain of several weeks' or months' duration that is often poorly localized to the thigh, the groin or the knee. Hip pain is reported less frequently. Often, a vague history of antecedent trauma calls attention to the limp and pain. As the epiphysis continues to slip, the child loses hip motion, including internal rotation, flexion and abduction. Because of this loss of motion, the child and the parents often describe a progressive external rotation and shortening of the lower extremity. This description is often accompanied by complaints of increasing difficulty in sports or in the performance of certain daily tasks, such as tying shoes.
Children with a minimal slipped capital femoral epiphysis experience only slight loss of internal rotation of the hip and have pain only at the extremes of motion. The gait is often antalgic; limb length discrepancy is not apparent, and muscle atrophy is minimal. As the slipped capital femoral epiphysis becomes more severe, the child's gait becomes more antalgic, with obvious external rotation. Discrepancy in limb length and thigh atrophy become readily apparent. Over time, internal rotation decreases, and abduction and flexion of the hip increases, along with automatic external rotation of the lower extremity with flexion of the hip.
The knee examination is always normal (i.e., no swelling, instability, joint line tenderness, erythema or warmth), as is the distal neurovascular examination.
Unstable Slipped Capital Femoral Epiphysis
Children with unstable slipped capital femoral epiphysis present with extreme pain, often after sports-related trauma or a fall with a twisting injury, such as from a curb. Most children have no prior history of symptoms.
During the office examination, the child typically reclines on the examination table, unable to move, and refuses any passive motion of the limb by the physician. In fact, if a slipped capital femoral epiphysis is suspected, no passive motion should be attempted for fear of further displacing the epiphysis. The hip is typically held in a position of flexion, external rotation and abduction, similar to that seen in an elderly patient with a displaced hip fracture. Distal neurovascular examination is normal.
Radiographic Findings
Stable Slipped Capital Femoral Epiphysis
Any obese adolescent or preadolescent presenting to the physician with a history of a limp, and thigh, knee or groin pain of several weeks' to one month's duration should be presumed to have a slipped capital femoral epiphysis until proved otherwise. Anteroposterior and lateral radiographs of both hips must be taken to confirm or exclude the diagnosis. If the child presents with a stable hip, anteroposterior and frog-lateral pelvic radiographs should be obtained. If the child presents with an unstable hip, an anteroposterior pelvic radiograph, a cross-table lateral radiograph of the involved hip and either a frog-lateral or a cross-table lateral radiograph of the opposite hip are recommended.
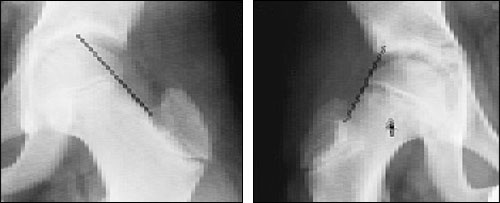
Often, early in the course of a slipped capital femoral epiphysis, the anteroposterior radiograph is normal since the initial early slippage is posterior. Consequently, a lateral radiograph must always be obtained. The early sign seen on the lateral radiograph is a minimal posterior step-off at the anterior epiphyseal-metaphyseal junction, or physeal plate (Figure 1). On anteroposterior radiographs, subtle early signs include Klein's line and the blanch sign of Steel.5 Klein's line is a line drawn along the superior surface of the femoral neck. The epiphysis should normally project superiorly to it (Figure 2, left), whereas in early slipped capital femoral epiphysis, the epiphysis is flush with it (Figure 2, right). The blanch sign of Steel on the anteroposterior radiograph represents superimposition of the posteriorly displaced epiphysis on the femoral neck (Figure 2, right).

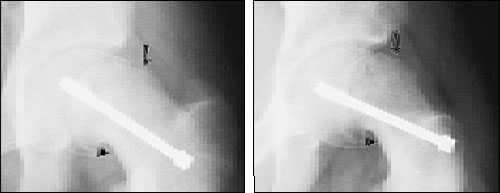
As the slip continues, there is further inferior and posterior displacement of the epiphysis relative to the metaphysis. The body attempts to remodel this displacement, smoothing away the superior and anterior portion of the proximal metaphysis (femoral neck). The skeleton also responds by forming callus (healing bone) at the inferior and posterior portions of the proximal metaphysis in an attempt to structurally buttress the slippage (Figure 3).
Unstable Slipped Capital Femoral Epiphysis
A patient with an unstable slipped capital femoral epiphysis has an abrupt displacement at the physeal plate, with posterior and inferior slippage of the epiphysis. In the traditional acute-on-chronic classification, some of the remodeling changes described above may be evident, but usually the patient has no prior history of symptoms and no visible remodeling of the proximal metaphysis (Figure 4). These children are often in such pain that only a single projection of the hip can be obtained, usually an anteroposterior radiograph.

Slip Severity
Two methods are commonly used to describe the radiographic magnitude of slip severity.1,6,7 The first method involves the amount of relative displacement of the epiphysis on the metaphysis. In a patient with a mildly slipped capital femoral epiphysis, the amount of displacement is less than one third; in a patient with a moderately slipped capital femoral epiphysis, the amount of displacement is from one third to one half, and in a patient with a severely slipped capital femoral epiphysis, the amount of displacement is greater than one half. In a patient with a stable slipped capital femoral epiphysis of many months' duration, remodeling of the femoral neck can make this classification difficult and less reliable, often leading to underestimation of the true magnitude of the slip.
Because of concerns with this semi-quantitative classification method, the epiphyseal-shaft angle of Southwick has been used to characterize slip severity (Figure 5). Although this angle takes slightly longer to measure than the amount of relative displacement of the epiphysis on the metaphysis, it is a more accurate reflection of the true magnitude of slippage. The angle is measured on the frog-lateral radiograph of the pelvis. A line is drawn between the anterior and posterior tips of the epiphysis at the physeal plate level; then a perpendicular line is drawn to this epiphyseal line. Next, a line is drawn along the mid-axis of the femoral shaft. The epiphyseal-shaft angle is the angle formed by the intersection of the perpendicular line and the femoral shaft line. It is measured for both hips, and the magnitude of slip displacement is the angle of the involved hip minus the angle of the contralateral normal hip. Using the measurement of this angle, a slipped capital femoral epiphysis can be classified as mild (less than 30 degrees), moderate (from 30 to 50 degrees) or severe (greater than 50 degrees). If involvement is bilateral, 12 degrees can be used as the control angle.
Treatment
The goals of treatment are to prevent further slippage and to achieve closure of the physeal plate. Although reduction of a slipped capital femoral epiphysis seems to be teleologically reasonable, it is disastrous in the stable patient since it is likely to cause avascular necrosis. Once a diagnosis is made, the child should immediately be made non-weight bearing, placed on crutches or in a wheelchair, and referred to an orthopedic surgeon. Prolonged non-weight bearing with crutches or a wheelchair does not constitute treatment, since the epiphysis invariably continues to slip. Definitive treatment should be performed as soon as possible and is best if performed within a few days. Use of crutches or a wheelchair minimizes the chance of a child falling and creating an unstable slipped capital femoral epiphysis.
Stable Slipped Capital Femoral Epiphysis
There are many options for the treatment of stable slipped capital femoral epiphysis. These include internal fixation (pinning) in situ with either a single central screw or multiple pins and/or screws,6–8 bone-graft epiphyseodesis,9,10 corrective osteotomy11,12 and spica cast immobilization.13,14 Most orthopedic surgeons currently recommend in situ fixation with a single central screw (Figure 3). The results of this technique have been excellent. Morbidity, complications and blood loss are minimal because of advances in intraoperative fluoroscopy and the development of strong implants that can be surgically placed using cannulated techniques. In situ fixation can usually be performed through a small incision with essentially no blood loss or wound complications. Failure of the fixation to hold the epiphysis, resulting in further slippage, is extremely rare in patients with a stable slipped capital femoral epiphysis and is no higher than the failure rate of other methods. Postoperatively, toe-touch weight bearing with crutches is recommended for four to six weeks, followed by a gradual return to normal activities. Once physeal closure has occurred, running and contact sports may be resumed. Removal of the internal fixation is a matter of controversy; some orthopedic surgeons recommend it, while others do not.
Although popular in the past, the use of multiple pins and screws is becoming less popular. The risk of intra-articular pin penetration is much higher than the risk of penetration with a single central screw. Pin penetration can cause articular cartilage damage and increases the risk of chondrolysis.
Bone graft epiphyseodesis, although resulting in a more rapid closure of the physis,9 has a higher complication rate, including graft breakage and further slippage, increased blood loss and more wound complications.10 Corrective osteotomy in the more severe cases of slipped capital femoral epiphysis, although more anatomically sound, is a much more invasive surgery with the potential for nonunion and hardware failure, and large incisions with blood loss and wound complications.1,15 Most importantly, the use of corrective osteotomy is associated with a much higher rate of the two most serious complications of slipped capital femoral epiphysis: avascular necrosis and chondrolysis.15,16
Unstable Slipped Capital Femoral Epiphysis
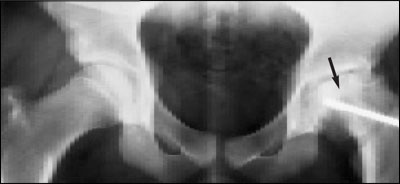
Because of the abrupt nature of the slippage, children with unstable slipped capital femoral epiphyses have a much higher rate of avascular necrosis related to disruption of epiphyseal vascularity (Figure 6). Nearly all orthopedic surgeons recommend internal fixation for unstable slipped capital femoral epiphyses. However, controversy exists regarding the timing of the surgery (immediate fixation versus fixation a few days after diagnosis); the number of screws and/or pins to be used; whether a reduction should be performed, and whether preliminary traction should be used.16 Since this type of slipped capital femoral epiphysis is rare, not enough data are currently available to convincingly answer these questions.
Prognosis
Barring the complications of avascular necrosis or chondrolysis, the prognosis for the child with a slipped capital femoral epiphysis remains good. Degenerative hip arthritis will develop gradually over several decades. This risk increases and occurs earlier according to the severity of the slipped capital femoral epiphysis,1 which explains why early diagnosis is so crucial. In long-term studies,1 results of in situ fixation techniques were better than results of realignment osteotomy.
However, the surgical techniques and fixation methods used today are far superior to those used in those long-term studies. The results of osteotomy using today's surgical techniques compared with results using today's methods of in situ fixation will not be known for at least three decades.
Avascular necrosis is the most serious complication of slipped capital femoral epiphysis.17 Children with avascular necrosis exhibit a more rapid arthritic deterioration of the hip and require reconstructive procedures such as hip fusion and total hip replacement earlier in adulthood; occasionally, reconstructive procedures are necessary even during adolescence.18
Chondrolysis occurs in approximately 5 to 7 percent of all children with slipped capital femoral epiphyses, even before treatment.17 The incidence of chondrolysis increases as the severity of the slipped capital femoral epiphysis increases, again underscoring the need for a rapid and accurate diagnosis. Clinically, children with chondrolysis demonstrate pain and loss of hip motion out of proportion to the severity of the slipped epiphysis. A loss of articular cartilage width can be seen on radiographs. Treatment is difficult and often fails. In approximately one half of children, the joint space gradually reconstitutes, with no significant worsening of long-term prognosis. In other children, chondrolysis may progress to such severe pain and contracture that hip arthrodesis is needed.