Functional endoscopic sinus surgery is a minimally invasive technique used to restore sinus ventilation and normal function. The most suitable candidates for this procedure have recurrent acute or chronic infective sinusitis, and an improvement in symptoms of up to 90 percent may be expected following the procedure. Fiberoptic telescopes are used for diagnosis and during the procedure, and computed tomography is used to assess the anatomy and identify diseased areas. Functional endoscopic sinus surgery should be reserved for use in patients in whom medical treatment has failed. The procedure can be performed under general or local anesthesia on an outpatient basis, and patients usually experience minimal discomfort. The complication rate for this procedure is lower than that for conventional sinus surgery.
Functional endoscopic sinus surgery (FESS) is a minimally invasive technique in which sinus air cells and sinus ostia are opened under direct visualization. The goal of this procedure is to restore sinus ventilation and normal function.1–4
The ability to treat paranasal sinus disease has been revolutionized by fiberoptic endoscopes and computed tomographic (CT) scanning. Fiberoptic endoscopes have made it possible to examine the nose thoroughly from the anterior nares to the postnasal space. The endoscopic procedure requires local anesthetic and may be performed in the office (Figures 1 through 3). The specific features that must be identified and assessed during the examination are the middle turbinate and the middle meatus (osteomeatal complex), anatomic obstruction, mucopus and nasal polyps (Figures 4 through 6).
FIGURE 1.

A patient undergoing nasal endoscopy.
FIGURE 2.
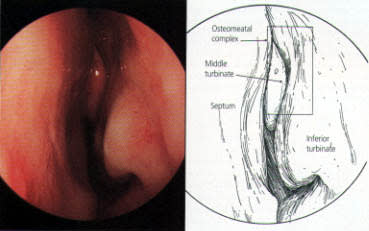
Endoscopic appearance of the left nostril in a normal nose. The septum is visible to the left, and the inferior turbinate and middle turbinates are also visible.
FIGURE 3.
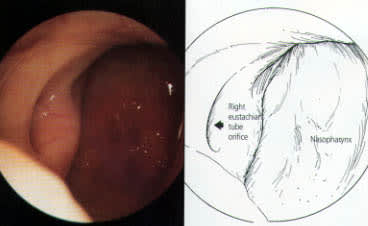
Endoscopic view of the normal postnasal space. The right eustachian tube orifice is visible to the left.
FIGURE 4.
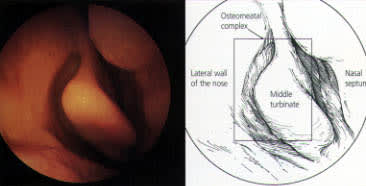
Endoscopic view of the normal middle turbinate, looking into the right nostril. The septum is to the right, with the lateral wall of the nose to the left.
FIGURE 5.
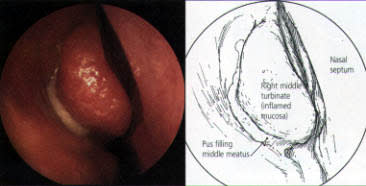
Endoscopic appearance of acute infective sinusitis, with pus exuding from under the right middle turbinate and down into the middle meatus.
FIGURE 6.
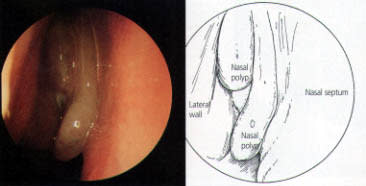
Nasal polyps in the left nostril, blocking the osteomeatal complex.
CT scanning identifies the anatomic relationships of the key structures (orbital contents, optic nerve and carotid artery) to the diseased areas, a process that is vital for surgical planning. CT also defines the extent of disease in any individual sinus, as well as any underlying anatomic abnormalities that may predispose a patient to sinusitis (Figures 7 through 10).
FIGURE 7.
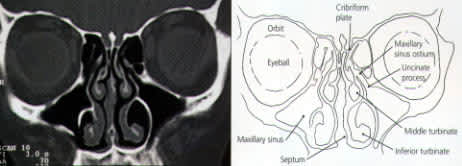
Coronal computed tomographic scan showing normal osteomeatal complex. Patent ostia are visible on both sides, and sinuses are well ventilated.
FIGURE 8.
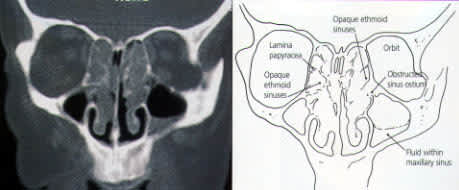
Coronal computed tomographic scan showing ethmoidal polyps. Ethmoid opacity is total as a result of nasal polyps, with a secondary fluid level in the left maxillary antrum.
FIGURE 9.
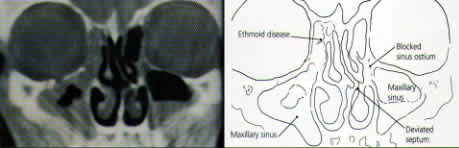
Coronal computed tomographic scan showing rhinosinusitis with a blocked osteomeatal complex and secondary infection in the maxillary sinuses.
FIGURE 10.
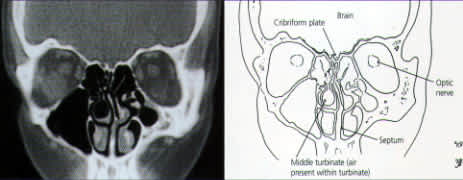
Coronal computed tomographic scan showing developed right middle turbinate (concha bullosa) and a deviated nasal septum.
The reasoning and concepts supporting the use of FESS have recently become widely accepted. (The term “functional” was introduced to distinguish this type of endoscopic surgery from nonendoscopic, “conventional” procedures.3,4) The goal of FESS is to return the mucociliary drainage of the sinuses to normal function. The paranasal sinuses are maintained in a healthy state by ventilation through the individual ostia and by a mucociliary transport mechanism that keeps a continuous protective layer of mucus flowing out of the sinuses.
Pathophysiology of Sinusitis
All of the sinuses need ventilation to prevent infection. In the normal state, this ventilation is provided through openings (ostia) into the nose (Figures 11 and 12). The natural ostia open into the middle meatus under the middle turbinate, with the exception of the posterior ethmoid air cells and the sphenoid sinus, which have ostia situated more posteriorly. Cilial activity in the sinuses directs the flow of mucus toward these ostia. The middle turbinate and the middle meatus together represent the key area of the nose, known as the osteomeatal complex.
FIGURE 11.
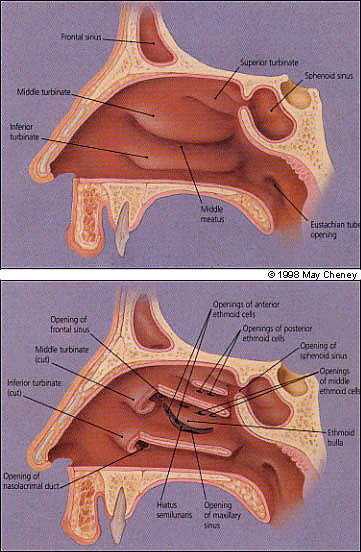
(Top) Lateral nasal wall (right side) showing turbinates and frontal sphenoid sinuses. (Bottom) Lateral nasal wall (right side), turbinates cut.
FIGURE 12.
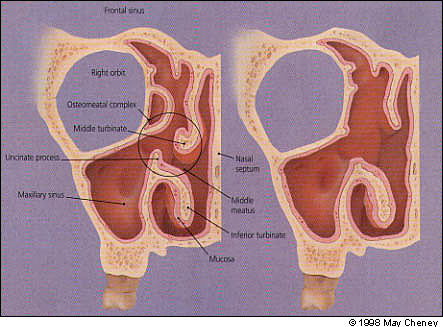
Anatomy of the sinuses. (Left) Narrowing in the circled region (middle meatus, middle turbinate, uncinate process) may precipitate sinusitis. (Right) After functional endoscopic sinus surgery, the osteomeatal area is open.
Most cases of sinusitis are caused by a problem in the nose (rhinogenic). Occasionally another problem, such as a primary dental infection, leads to sinusitis. During any episode of rhinosinusitis, the cilia function less efficiently, resulting in mucus stasis. The nasal sinus mucosa become engorged, often closing the ostia. A poorly ventilated sinus is the result, and the hypoxia and mucus stasis produce ideal conditions for bacterial infection.
Initial Evaluation and Treatment
As with many disease processes, the history of a patient with sinusitis is probably the most important part of the preoperative assessment (Table 1). All patients with severe or persistent symptoms should be evaluated, and many can be helped with advice and medical treatment.
TABLE 1 Symptoms of Rhinosinusitis
| Nasal obstruction |
| Sinofacial pain or headache |
| Mucopurulent rhinorrhea and postnasal drip |
| Sneezing |
| Reduced sense of smell and taste |
The fiberoptic endoscope enables the surgeon to examine the nose in great detail and is an essential tool for diagnosis. Patients with seasonal or perennial rhinitis should be given advice about avoidance of allergens and treatment with topical nasal steroid sprays and antihistamines. Acute infective sinusitis is treated with antibiotics and vasoconstrictor nasal sprays. If medical treatment has failed, the patient may be a suitable candidate for an endoscopic procedure.
Candidates for Sinus Surgery
FESS (like any sinus surgery) is most successful in patients who have recurrent acute or chronic infective sinusitis. Patients in whom the predominant symptoms are facial pain and nasal blockage usually respond well. The sense of smell often improves after this type of surgery.
A CT scan before FESS is mandatory to identify the patient's ethmoid anatomy and its relationship to the skull base and orbit. CT scanning also allows the extent of the disease to be defined, as well as any underlying anatomic abnormalities that may predispose a patient to sinusitis.
Patient selection therefore involves a thorough history and physical examination, a trial with medical treatment and, finally, CT scanning. The result is a highly selected group of patients who can expect an improvement of up to 90 percent in their symptoms.
In patients with nasal polyposis that is not controlled with topical corticosteroids, FESS permits the accurate removal of polyps using suction cutters.5 It is not known whether the disease-free interval is extended for patients having endoscopic ethmoidectomies for polyposis compared with conventional polyp surgery, but the postoperative discomfort is minimal.
Nonendoscopic, ‘Conventional’ Sinus Surgery vs. FESS
It was previously believed that once the mucosa had become chronically inflamed, it was irreversibly damaged and had to be removed. This was the rationale behind the Caldwell-Luc surgical technique, which involves removal of the diseased lining of the maxillary antrum (Figure 13). Similarly, the external surgical approaches to the ethmoid and frontal sinuses were designed to be “radical operations” in which the disease was completely cleared. These procedures left scars and caused significant bruising and discomfort. The Caldwell-Luc procedure also caused numb teeth. These “conventional procedures,” as well as the sinus washout, concentrate on the secondarily infected sinus while ignoring the important pathology within the nose.
FIGURE 13.

Patient undergoing Caldwell-Luc surgery, involving removal of the diseased lining of the maxillary antrum.
The rationale behind FESS is that localized pathology in the osteomeatal complex blocks the ostia and leads to inflammation in the dependent sinuses (Figure 12). The surgical interventions of the procedure are designed to remove the osteomeatal blockage and restore normal sinus ventilation and mucociliary function (Figure 12).
FESS, like all minimally invasive surgery, is designed to combine an excellent outcome with minimal patient discomfort. As mentioned, the main advantage of FESS compared with traditional techniques is that it is less invasive, resulting in minimal postoperative discomfort. Scars and damage to the nerve supply of the teeth are also avoided. The use of the endoscope permits a better view of the surgical field, and this is probably responsible for the lower rate of complications.
The focal point of the surgery is the osteomeatal complex. The procedure may be performed with local anesthesia, with or without sedation. FESS is suitable for outpatient surgery.
Surgical Technique
After suitable vasoconstriction using cocaine or ephedrine, the middle turbinate is identified. This is the most important landmark for the procedure. On the lateral wall of the nose at the level of the anterior end of the middle turbinate lies the uncinate process. This is removed (Figure 14), exposing the ethmoid bulla and the opening called the hiatus semilunaris, into which the frontal and maxillary sinuses drain.
FIGURE 14.
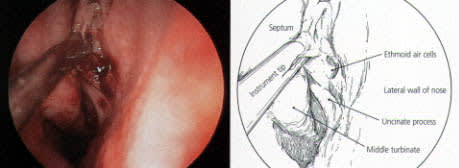
Surgical removal of the uncinate process.
The anterior ethmoid air cells are then opened, allowing better ventilation but leaving the bone covered with mucosa. Following this, the maxillary ostium is inspected and, if obstructed, opened by means of a middle meatal antrostomy (Figure 15). This minimal surgery will often be sufficient to greatly improve the function of the osteomeatal complex and therefore provide better ventilation of the maxillary, ethmoid and frontal sinuses.
FIGURE 15.
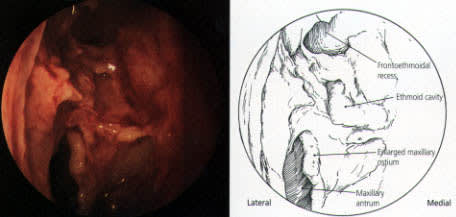
A middle meatal antrostomy in the right nostril.
Occasionally the CT scan shows disease in the posterior ethmoids and the sphenoid sinus. It is then necessary to continue further into these sinuses. However, in most cases of sinusitis, the inflammation is confined to the osteomeatal complex and the anterior ethmoids.
Postoperative Care
Postoperatively, it is important to keep the nose as free from build-up of crusts as possible. The techniques used to achieve this vary from time-consuming nasal toilet performed two to three times a week by the surgeon to simple nasal douching carried out several times a day by the patient. Normal function usually returns within one to two months. In patients with gross inflammation or polyps, a short course of systemic steroids combined with antibiotics may hasten postoperative recovery. Topical steroids are used postoperatively in patients who have had polyps removed.
Outcome
The results after FESS are good, with most studies reporting an 80 to 90 percent rate of success.6–9 Good results also have been obtained in patients who have had previous sinus surgery.
The procedure is considered successful if the majority of the patient's symptoms are resolved. Nasal obstruction and facial pain are most likely to be relieved, although postnasal drip often remains a challenge. The technique has been compared with the Caldwell-Luc procedure and, although both methods were found to be effective, there was a strong patient preference for FESS.10 The extent of disease affects the outcome, with the best results obtained in patients with limited nasal pathology producing secondary sinusitis.11
Complications
The most catastrophic complication of FESS is blindness resulting from damage to the optic nerve. However, the evidence indicates that the frequency of this complication is extremely low.12,13
Cerebrospinal fluid leak is the single most common major complication of FESS, occurring in about 0.2 percent of cases.13 The leak is usually recognized at the time of surgery and can easily be repaired; it should be suspected if there is a clear nasal discharge postoperatively. Unless the discharge is contaminated with blood, the presence of glucose means that it is most likely to be cerebrospinal fluid. Absolute confirmation may be obtained by having a sample tested for the presence of beta2 transferrin.
Other, less serious, but still rare complications include orbital hematoma and nasolacrimal duct stenosis. It should be emphasized that all of these complications also may occur with “conventional” sinus surgery and, therefore, patients are not undergoing a new treatment with complications that are more serious or more frequent than those in other surgeries. In the United Kingdom, the overall major complication rate of FESS was 0.44 percent, compared with 1.4 percent in patients having similar, nonendoscopic procedures.13
Extended Uses of FESS
Endoscopic Dacryocytorhinostomy
This procedure is usually performed by an otolaryngologist and an ophthalmic surgeon working together. It can be performed with local anesthetic during an office visit. The blockage within the tear duct is confirmed with a contrast dacryocystogram. The ophthalmic surgeon dilates the duct and passes a fine flexible fiberoptic light lead down the duct so that the endoscopic surgeon can identify the light in the lateral wall of the nose, usually just in front of the middle turbinate. The endoscopist uses a microdrill or laser to remove the bone overlying the duct. Stents are inserted and left in place for six weeks. The success rate is equal to rates with external dacryorhinostomy (80 to 90 percent), and an external incision is avoided.14
Endoscopic Orbital Decompression
Indications for endoscopic orbital decompression include optic neuropathy and the problems associated with the exophthalmos of thyroid eye disease (Figure 16). Endoscopic decompression of the orbit is achieved by first fully removing the ethmoid air cells and then removing the thin bone (lamina papyracea) that forms the medial wall of the orbit. The medial portion of the orbital floor may also be removed. If necessary, the thick bone that directly overlies the optic nerve at the orbital apex may be removed with a microdrill. Once fully exposed, the orbital periosteum is longitudinally incised, allowing the orbital fat to prolapse into the ethmoid cavities. A 4- to 5-mm reduction in proptosis is usually obtained, and this rate compares favorably with decompression methods that rely on external incisions.15
FIGURE 16.
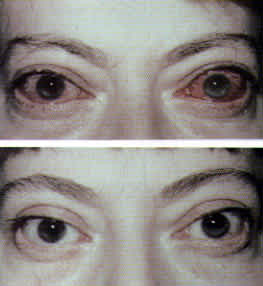
A patient with exophthalmos of thyroid eye disease before (top) and after (bottom) surgery to reduce proptosis and inflammation.
Access to Areas Otherwise Difficult to Reach
The endoscope permits access to areas that are difficult to view with conventional techniques, e.g., the sphenoid sinus. It is possible to drain most frontal, ethmoidal or sphenoidal mucoceles. Small pituitary tumors also may be removed endoscopically.
Limitations of FESS
Acute Severe Ethmoid and Frontal Sinusitis
Pus from an acute ethmoid sinusitis (Figure 17) may break through the lamina papyracea and cause a painful proptosed eye with a risk of loss of vision. If the response to intravenous antibiotics is not very rapid, urgent orbital decompression is required. Bleeding is likely to occur because of the acute inflammation, making endoscopic surgery extremely difficult. An ethmoidectomy via an external incision may be the preferable option.
FIGURE 17.

A patient with acute ethmoiditis threatening vision.
Severe frontal sinusitis may be associated with intracranial sepsis and under these circumstances, a direct trephine into the frontal sinus together with the appropriate neurosurgical intervention is the best option.
Nasal and Sinus Malignancies
Nasal and sinus malignancies are rare and often present late. If radical surgery is indicated, it is best performed via an external approach, such as midfacial degloving, lateral rhinotomy and various craniofacial procedures. However, the endoscope is useful for diagnosis and biopsy of tumors and for monitoring patients who have had radical cancer surgery.
