
This is a corrected version of the article that appeared in print.
Am Fam Physician. 2000;61(9):2683-2690
A more recent article on preparticipation physical evaluations is available.
A comprehensive medical history that includes questions about a personal and family history of cardiovascular disease is the most important initial component of the preparticipation athletic evaluation. Additional questions should focus on any history of neurologic or musculoskeletal problems. A limited physical examination should emphasize cardiac auscultation with provocative maneuvers to screen for hypertrophic cardiomyopathy. This condition is the most common cause of sudden death in young male athletes. Other components of the physical examination include an evaluation of the spine and extremities. Screening tests such as electrocardiography, treadmill stress testing and urinalysis are not indicated in the absence of symptoms or a significant history of risk factors. Specific conditions that would exclude or limit athletic participation include hypertrophic cardiomyopathy, long QT interval syndrome, concussion, significant knee injury, sickle cell disease and uncontrolled seizures. Overall, about 1 percent of athletes who are screened are completely disqualified from sports participation.
The overall rate of sudden death in male athletes younger than 35 years is quite low, approximately 0.75 per 100,000 participants per year.1 Congenital cardiac anomalies account for most sudden deaths in these patients. The most common anomalies are hypertrophic cardiomyopathy and coronary artery anomalies.1
The most common coronary abnormality is a left main coronary artery originating off the right sinus. Myocarditis, rupture of the aorta, arrhythmogenic right ventricular dysplasias, idiopathic left ventricular hypertrophy, aortic stenosis and premature coronary artery disease account for most of the remaining fatalities.2
When large groups of young athletes are evaluated, few are disqualified because these disorders are suspected. Rather, the most common abnormalities leading to disqualification are musculoskeletal conditions, followed by other cardiac problems.3 Even when cardiac abnormalities are detected, the leading disqualifiers are rhythm and conduction abnormalities, systemic hypertension and valvular heart disease,4 not the cardiac abnormalities listed in the opening paragraph.
Screening History
CARDIOVASCULAR
The personal and family history of the athlete reveals 64 to 78 percent of conditions that could prohibit or alter sports participation, making it a more sensitive tool than the physical examination.5
The history more reliably detects risk factors and symptoms of coronary artery disease in older athletes than in younger athletes.2 Hypertrophic cardiomyopathy, the most common cause of death among 12- to 32-year-old athletes on the field, may not produce symptoms before sudden death.6 All potential athletes should be asked about previous injuries and levels of physical activity. The latter information is particularly important in a potential athlete more than 35 years of age who has been sedentary and is now contemplating a vigorous exercise program.
A personal history of congenital or acquired heart disease, as well as a history of hypertension or murmurs, should be noted. Symptoms of chest discomfort, shortness of breath, palpitations, syncope or near-syncope with exercise are important. A known family history of hypertrophic cardiomyopathy, Marfan syndrome or atherosclerosis (especially premature), as well as a history of unexplained sudden death in family members younger than 50 years, are all of concern.
Hypertrophic cardiomyopathy is a heterogeneous group of disorders acquired through autosomal dominant transmission with incomplete penetrance, and signs and symptoms may not become manifest until early adulthood.7 Detecting persons with Marfan syndrome before they participate in sports is important because the defective aortic media can rupture during basketball, volleyball and, presumably, other sports activities.8 Table 1 is a representative checklist of historical cardiovascular questions to ask in the preparticipation examination. The patient giving an affirmative answer to any of these questions would merit a more detailed assessment.
| Exertional chest pain or discomfort, or shortness of breath? |
| Exertional syncope or near-syncope, or unexpected fatigue? |
| Past detection of cardiac murmur or systemic hypertension? |
| Known family history of hypertrophic cardiomyopathy, other cardiomyopathies, long QT syndrome, Marfan syndrome, significant dysrhythmias? |
| Family history of premature death or known disabling cardiovascular disease in a first- or second-order relative younger than 50 years? (More concern if younger than 40 years.) |
NEUROLOGIC
A report of burning pain, weakness, numbness or tingling in all four or only the upper extremities raises concerns of cervical spine impingement. Possible etiologies for this condition would include atlantoaxial instability, congenital fusions and disk herniations.
Medications and Substance Abuse
A medication history provides clues to current medical conditions, as well as a bridge into inquiries about nutritional supplements. Asking about the use of cocaine or anabolic steroids is particularly appropriate during a preparticipation physical examination because of the known cardiotoxic effects of these drugs.9 Eliciting information about patterns and amounts of alcohol use and the potential to be in an automobile with drunken drivers is appropriate in view of the overall mortality associated with these issues in the young adult population. Although alcohol use and the likelihood of riding with drunken drivers have nothing to do with the ability to participate in sports, this is a good opportunity to address these issues with young athletes.
Female Athletes
The American Heart Association does not recommend any gender-specific cardiovascular alterations in the screening of female athletes.2 Young women are even less likely to experience sudden death on the athletic field than young men; women account for only about 15 percent of such deaths.2 In female athletes, however, several predispositions should be considered.
Anorexia nervosa and other eating disorders are more common among female athletes than among male athletes. Screening questions about desires to change weight or displeasure with body habitus identify many of these women. Female runners are 12 times more likely to develop stress fractures than are male runners.10 Osteoporosis occurs in amenorrheic female athletes and its finding should prompt further consideration of the possibility of an eating disorder. Women who play soccer and basketball are also more susceptible to patellofemoral syndrome, foot disorders (i.e., hammertoes, bunions, plantar fasciitis), stress fractures to the forefoot, and anterior cruciate ligament injuries.11,12
Preparticipation Physical Examinations
The purpose of these examinations is to detect conditions that put the proposed athlete at risk for sudden death, but they have not been shown to be highly effective in this regard.13 A recent Italian study4 showed potential benefits in preventing sudden deaths when persons with certain conditions were disqualified (e.g., physical features of Marfan syndrome; delayed femoral arterial pulses; single, wide or fixed splits in the second heart sound; systolic or diastolic murmurs of grade 2/6 or greater; irregular rhythms; or blood pressures greater than 145/90 mm Hg). This study raises the issue of whether efforts to provide national screening and standards would be effective in the United States.
Table 2 presents the components of an appropriate physical examination. Individual alterations are appropriate, especially if the physician has had recent contacts with or recently examined the athlete, or has knowledge of the athlete's previous injuries and family history. Several items on the examination merit additional attention. Blood pressure must be interpreted on the basis of the patient's age, gender and height. For example, taller children may have higher readings and still be normotensive. Table 3 offers representative values, and the National High Blood Pressure Education Program's update on high blood pressure in children and adolescents offers more detailed coverage of this topic.14
| Examination feature | Comments |
|---|---|
| Blood pressure | Must be assessed in the context of participant's age, height and sex (see Table 3). |
| General appearance | Measure for excessive height and observe for evidence of excessive long-bone growth (arachnodactyly, arm span > height, pectus excavatum) that suggest Marfan syndrome. |
| Eyes | Important to detect vision defects that leave one of the eyes with > 20/40 corrected vision. Lens subluxations, severe myopia, retinal detachments and strabismus are associated with Marfan syndrome. |
| Cardiovascular | Palpate the point of maximal impulse for increased intensity and displacement that suggest hypertrophy and failure, respectively. |
| Perform auscultation with the patient supine and again with the patient standing or straining during Valsalva's maneuver. | |
| Femoral pulse diminishment suggests aortic coarctation. | |
| Respiratory | Observe for accessory muscle use or prolonged expiration and auscultate for wheezing. Exercise-induced asthma will not produce manifestations on a resting examination and requires exercise testing for diagnosis. |
| Abdominal | Assess for hepatic or splenic enlargement. |
| Genitourinary | Hernias and varicoceles do not usually preclude sports participation, but the sports examination can also serve as an appropriate time to screen for testicular masses if the athlete is not receiving regular general examinations. |
| Musculoskeletal | The two-minute orthopedic examination (see Appendix, p. 2696) is a commonly used systematic screen. Consider supplemental shoulder, knee and ankle examinations. |
| Skin | Evidence of molluscum contagiosum, herpes simplex infection, impetigo, tinea corporis or scabies would temporarily prohibit participation in sports where direct skin-to-skin competitor contact occurs (e.g., wrestling, martial arts). |
| Age (years) | Blood pressure (mm Hg) | |||||
|---|---|---|---|---|---|---|
| Girls | Girls | Boys | Boys | |||
| 50th percentile for height | 75th percentile for height | 50th percentile for height | 75th percentile for height | |||
| 6 | 111/73 | 112/73 | 114/74 | 115/75 | ||
| 12 | 123/80 | 124/81 | 123/81 | 125/82 | ||
| 17 | 129/84 | 130/85 | 136/87 | 138/88 | ||
Dynamic auscultation of the heart is critical in the detection of hypertrophic cardiomyopathy. In patients with this disorder, a soft systolic murmur along the left sternal border may be appreciated only when the patient stands up or during the straining phase of the Valsalva's maneuver, as these maneuvers decrease preload and the end diastolic volume of the left ventricle. Table 4 summarizes potential physical findings in patients with hypertrophic cardiomyopathy.
| Finding | Significance | |
|---|---|---|
| Systolic murmur | Turbulent flow of blood through a dynamic outflow tract obstruction. The murmur increases with activities that decrease the end diastolic volume of the left ventricle. | |
| Second right intercostal space and/or left sternal border | ||
| Murmur increases with standing and decreases with squatting | ||
| May radiate to neck | ||
| Lateral displacement of apical impulse | Hypertrophy and failure of left ventricle | |
| Holosystolic murmur of mitral regurgitation at apex with radiation to axilla | Malposition of mitral valve during systole, which interferes with valve closure | |
Ancillary Studies
ELECTROCARDIOGRAPHY
Routine screening use of 12-lead electrocardiography (ECG) for preparticipation physical examinations of high school and collegiate athletes is not recommended by the American Heart Association or other organizations.
In a normal, well-conditioned young athlete, the heart may develop ECG changes that falsely suggest ventricular hypertrophy; the specificity of the test is poor in this population.2 Nevertheless, selective use of ECG can be useful in assessing young athletes who, on the grounds of history, family history or physical examination, are thought to be at potentially higher risk.
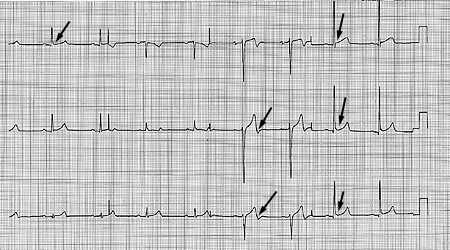
The resting ECG rate is abnormal in 80 to 90 percent of patients with hypertrophic cardiomyopathy, coronary anomalies and right ventricular dysplasias, as well as long QT interval syndrome. Figure 1 demonstrates a typical ECG from a patient with hypertrophic cardiomyopathy. The most common ECG abnormalities in patients with this condition are voltage criteria for left ventricular hypertrophy, abnormal ST-segments, T-wave inversion and deep Q waves.
ECHOCARDIOGRAPHY
Two-dimensional echocardiogrphy remains the diagnostic study of choice for detection of hypertrophic cardiomyopathy when the history and physical examination raise a suspicion of this disorder. Because hypertrophic cardiomyopathy represents a heterogeneous group of disorders, DNA testing is not a practical substitute. Echocardiograms can also confirm valvular pathology and demonstrate left ventricular dysfunction, aortic root dilatation and sometimes even aberrant origins of the left main coronary artery. They are not cost effective in large-scale general screening programs. Problems with false-positive results (e.g., enlargement in left ventricular wall thickness that occurs as a normal physiologic adaptation in the athlete) and false-negative results (e.g., hypertrophic cardiomyopathy may not demonstrate septal thickening until the end of adolescence) can occur.2
EXERCISE STRESS TESTING
Exercise stress testing has also not been shown to be cost effective in large screening programs of young athletes. It is appropriate in the older athlete with known coronary artery disease or when symptoms suggest stable angina or exercise-induced anginal variants. Table 515 presents stress test exercise levels that are associated with less risk of sudden exercise-related cardiac events. Exercise stress testing is also appropriate when risk factors (e.g., hypertension, smoking, diabetes mellitus) are present and the patient is contemplating an increase in exercise intensity. The American College of Sports Medicine16 recommends exercise stress testing in men older than 40 years and women older than 50 years before starting a vigorous exercise program.
| Age (years) | Threshold |
|---|---|
| < 50 | > 10 METS |
| 50 to 59 | > 9 METS |
| 60 to 69 | > 8 METS |
| > 70 | > 7 METS |
OTHER TESTS
The yield of urinalysis, complete blood counts and determination of serum ferritin levels is poor in asymptomatic, healthy sports participants. The results, even if abnormal, do not usually affect sports participation. These tests are not recommended in this setting.5
Medical Conditions and Sports
If the physician has identified a medical or orthopedic problem, the issue is whether to disqualify the athlete from the sport or allow the athlete to play with restrictions, with or without treatment. Most athletes are healthy; only 3 to 13 percent require further evaluation, and the disqualification rate for 10 million annual examinations is less than 1 percent.17
CARDIOVASCULAR DISEASES
A much more detailed assessment, often with specialist consultation, is required to define the nature and intensity of sports participation when conditions are discovered on screening. Some conditions that would prohibit any sports activity, or certain sports activities (as indicated by parentheses) are shown in Table 6. The potential for adverse outcomes cannot be clearly defined on the basis of whether a condition exists or not, but instead requires a more exact knowledge of the status of that condition. Although recent studies have shown that some patients with hypertrophic cardiomyopathy do not experience sudden premature death, 1 percent of persons diagnosed with the condition die of it each year.18
| Active myocarditis or pericarditis | |
| Hypertrophic cardiomyopathy | |
| Severe hypertension until controlled by therapy (static resistance activities, such as weight lifting, are particularly contraindicated) | |
| Suspected coronary artery disease until fully evaluated (patients with impaired resting left ventricular systolic function < 50%, or exercise-induced ventricular dysrhythmias, or exercise-induced ischemia on exercise stress testing are at greatest risk of sudden death) | |
| Long QT interval syndrome | |
| History of recent concussion and symptoms of postconcussion syndrome (no contact or collision sports) | |
| Poorly controlled convulsive disorder (no archery, riflery, swimming, weight lifting or power lifting, strength training or sports involving heights) | |
| Recurrent episodes of burning upper-extremity pain or weakness, or episodes of transient quadriplegia until stability of cervical spine can be assured (no contact or collision sports) | |
| Sickle cell disease (no high-exertion, contact or collision sports) | |
| Eating disorder where athlete is not compliant with therapy and follow-up, or where there is evidence of diminished performance or potential injury because of eating disorder | |
| Acute enlargement of spleen or liver | |
Cardiologist evaluation and clearance for a patient with hypertrophic cardiomopathy would be mandatory before any athletic participation. Survival is decreased in patients with advanced symptoms at the time of diagnosis, an obstruction gradient of more than 30 mm Hg, left ventricular wall thickness greater than 25 mm on ECG or associated atrial fibrillation.
Mitral valve prolapse (MVP) would not prohibit sports participation in the vast majority of patients. However, there is increased risk if MVP is associated with repetitive supraventricular dysrhythmias or ventricular dysrhythmias with a family history of sudden death, or with a history of embolism or marked mitral regurgitation; therefore, patients with these conditions should be limited to low-intensity sports.19 Sinus bradycardia and similar dysrhythmias are common in young athletes and, like non–exercise-induced ectopic beats, are not a basis for restriction in asymptomatic patients without structural heart disease.
Other dysrhythmias such as pre-excitation syndromes, atrial fibrillation, paroxysmal supraventricular tachycardia and ventricular tachycardia usually require that the athlete be asymptomatic, with documented control of the rhythm, for six months before sports participation can be approved. Associated structural problems with the heart or certain medications used to treat dysrhythmia-related conditions impose additional restrictions (e.g., no contact sports in a patient taking warfarin [Coumadin] for atrial fibrillation). The recommendations of the 26th Bethesda Symposium include a more detailed discussion of athletic participation in persons with cardiac abnormalities.19
MUSCULOSKELETAL INJURIES
Most studies have shown that musculoskeletal findings are the major category of abnormalities leading to restriction from sports activities.3 The most common musculoskeletal injury to restrict an athlete from activity is a knee injury, followed by an ankle injury.20 In knee injuries, the chance of reinjury is high without proper rehabilitation.21 If the athlete must actively use a joint in the sport for which he or she is seeking clearance, several criteria must be fulfilled. There should be no joint effusion, reduced range of motion or symptomatic ligament instability, and at least 80 to 90 percent of normal strength must be present in the affected extremity. Ligament laxity can be a normal physical finding or trait, but symptomatic instability is pathologic.
HEAD AND CERVICAL SPINE INJURY
Concussions are the most common injuries in football. There is no clear agreement on definitions or classifications of concussion severity, treatment or clearance guidelines.22 Individual assessment and clinical judgment should prevail. In general, however, athletes with a history of concussion who have been asymptomatic for at least one week and show no residual neurologic deficits are allowed to participate in sports.
Any persistent symptoms of postconcussion syndrome (headache, dizziness, sensory changes or mental difficulty) are a contraindication to contact sports, even though they may take weeks to resolve. This cautious approach may prevent fatal second-impact syndrome in athletes who have a second concussion while recovering from a first.23 The first concussion is believed to disrupt autoregulation of the brain's blood supply. If a second impact follows, vascular engorgement and increased intracranial pressure result, sometimes producing brain-stem herniation. This syndrome can occur even when the first concussion is mild, with symptoms of decreased alertness or postconcussion amnesia only.
“Burners” or “stingers” are usually secondary to a brachial plexus stretch or cervical root irritation. The athlete should be free of any neck or radicular pain, and have full range of motion and strength in all movements of the cervical spine before returning to sports participation.24 Recurrent episodes or transient quadriplegia requires cervical radiographic studies before clearance.
CONVULSIVE DISORDERS
Guidelines from the American Academy of Pediatrics (AAP) 25 clear young athletes with well-controlled convulsive disorders for participation in conventional school-sponsored sports. However, if a sport entails high risk (e.g., skiing, gymnastics, high diving), neurologic consultation should be considered. Athletes with poorly controlled seizures should be withheld from contact or collision sports and hazardous noncontact sports such as archery, riflery, swimming and weight lifting.
EXERCISE-INDUCED ASTHMA
Status asthmaticus is one of the nontraumatic causes of death in high school and college athletes. However, the incidence in survey populations is only four deaths in 30 million athletes.1 Evidence of exercise-induced asthma is sought in the preparticipation examination so that medical prophylaxis (typically with a beta agonist) can be implemented, not to disqualify the athlete.
HEAT-RELATED ILLNESS
Leading causes of nontraumatic, noncardiac sports death are exertional hyperthermia, followed by exertional rhabdomyolysis and status asthmaticus.1 Physicians can screen for a tendency toward exertional hyperthermia by asking about a previous history of heat-related illness. Athletes with this condition are usually allowed to participate in sports, but temperature extremes must be avoided, and hydration must be ensured.
SICKLE CELL TRAIT
The AAP and the National Collegiate Athletic Association recommend that persons with sickle cell trait be allowed to participate in sports without any restrictions.25 There is evidence that persons with sickle cell trait have increased susceptibility to exertional rhabdomyolysis, with the potential for renal failure and death. Patients with sickle cell trait should be counseled about appropriate hydration and acclimatization to reduce risks.
High exertion and contact or collision sports are generally contraindicated in patients with sickle cell disease, even if appropriate hydration can be ensured.
SOLITARY ORGANS
Whether athletes with one paired organ, especially one kidney, should participate in sports is a topic of controversy. All such patients need to understand the risks so they can make an informed decision. No contact or collision sports are allowed if a single kidney is polycystic or abnormally located.
When an athlete has only one functional eye (with less than 20/40 corrected visual acuity), further evaluation by an ophthalmologist is recommended.26 These athletes can participate only in sports (such as swimming, track and field, and gymnastics) that permit the use of protective eyewear and do not involve projected objects. Wrestling, boxing and martial arts are contraindicated sports.
The only modification for an athlete with one testicle is the use of a protective cup during contact sports. The chance of injury and the subsequent possibility of loss of fertility should be mentioned in counseling.
Final Comment
Although exercise-related sudden deaths in young athletes are rare, efforts to detect potential causes of such deaths are appropriate. Detection of solitary organs and preventive strategies for patients with this condition, especially those who are functionally uniocular, can avert morbidity. The preparticipation examination can achieve these goals and allow the family physician an opportunity to address the major health issues in young adults, such as alcohol and drug use, suicide, sexually transmitted diseases and pregnancy prevention.