Patients with acute brachial plexus neuritis are often misdiagnosed as having cervical radiculopathy. Acute brachial plexus neuritis is an uncommon disorder characterized by severe shoulder and upper arm pain followed by marked upper arm weakness. The temporal profile of pain preceding weakness is important in establishing a prompt diagnosis and differentiating acute brachial plexus neuritis from cervical radiculopathy. Magnetic resonance imaging of the shoulder and upper arm musculature may reveal denervation within days, allowing prompt diagnosis. Electromyography, conducted three to four weeks after the onset of symptoms, can localize the lesion and help confirm the diagnosis. Treatment includes analgesics and physical therapy, with resolution of symptoms usually occurring in three to four months. Patients with cervical radiculopathy present with simultaneous pain and neurologic deficits that fit a nerve root pattern. This differentiation is important to avoid unnecessary surgery for cervical spondylotic changes in a patient with a plexitis.
Acute brachial plexus neuritis is an uncommon disorder of unknown etiology that is easily confused with other neck and upper extremity abnormalities, such as cervical spondylosis and cervical radiculopathy.1–3 Patients with acute brachial plexus neuritis present with a characteristic pattern of acute or subacute onset of pain followed by profound weakness of the upper arm and amyotrophic changes affecting the shoulder girdle and upper extremity.1,2,4 In 1943, Spillane5 was probably the first to recognize acute brachial plexus neuritis as a distinct clinical entity. In 1948, Parsonage and Turner6 described 136 cases of this condition and, in view of the doubts of pathology and etiology at the time, gave it the name “neuralgic amyotrophy.”
Illustrative Case
A 66-year-old man presented with the complaint of severe, left-sided neck pain that radiated into the left shoulder, without associated numbness or tingling. Onset of the pain was one week earlier. Several weeks before he presented for examination, he had received an influenza vaccination. On initial physical examination, he exhibited normal strength, sensation and reflexes of the upper extremities. He subsequently developed weakness in the deltoid, infraspinatus and supraspinatus muscles. His sensory examination was within normal limits.
Cervical spine radiographs revealed cervical spondylosis. Magnetic resonance imaging (MRI) did not reveal nerve root compression on the left; however, it did reveal a spondylotic defect on the right at the C4-5 level and a bony ridge at the C5–6 level, causing foraminal narrowing that was greater on the right than on the left. The patient underwent evaluation with a myelogram, and a computed tomographic (CT) myelogram revealed osteophytes bilaterally at the C4–5 level and lesser spondylotic changes at the C3–4 level.
Cerebrospinal fluid studies revealed 1,045 red blood cells per mm3 (1,045 × 106 per L) with 3 nucleated cells per mm3 (3 ×106 per L), a glucose of 53 mg per dL (2.94 mmol per L), and a slightly elevated protein of 60 mg per dL (0.60 g per L).
Approximately three to four weeks after the onset of symptoms, the patient underwent an electromyogram and nerve conduction studies. The results were consistent with a diagnosis of brachial plexus neuritis with severe subacute denervation in the supraspinatus, infraspinatus and deltoid muscles. In particular, moderately severe spontaneous fibrillations and positive waves were evident in the deltoid, supraspinatus, infraspinatus and low cervical paraspinous muscles, and moderate, chronic repetitive discharges were noted in the levator scapulae muscles. With voluntary muscle activation, motor unit action potentials were of normal amplitude, duration and contour. Distal median and ulnar motor and sensory and radial sensory nerve conduction studies were within normal limits, as were proximal median and ulnar motor nerve conduction studies. A diagnosis of acute brachial plexus neuritis was made.
The patient was treated with a methylprednisolone dosepak (Medrol), hydrocodone and cyclobenzaprine (Flexeril). He underwent physical therapy for three weeks, and his condition slowly improved; however, he still experienced some mild difficulty with shoulder abduction for several months.
DISCUSSION
Pain in the cervical and shoulder area is common and may reflect a multitude of conditions. However, when a patient develops neurologic deficits, the list of differential diagnoses becomes shorter. Cervical radiculopathy is the most common condition. Patients with cervical radiculopathy present with cervical pain and neurologic deficits resulting from a herniated nucleus pulposus or an osteophyte. Acute brachial plexus neuritis mimics cervical radiculopathy in several aspects, but the treatments are significantly different.
Etiology and Epidemiology
Acute brachial plexus neuritis has been recognized as a distinct plexus disorder since the 1940s. Multiple names have been ascribed to it, including “brachial plexus neuropathy,” “local neuritis of the shoulder girdle,” “acute brachial plexitis,” “acute shoulder neuritis,” “paralytic neuritis” and “Parsonage-Turner syndrome.”
A viral etiology has been proposed, while other studies have emphasized that various infections precede the onset of acute brachial plexus neuritis in as many as 25 percent of cases.3,7,8 Up to 15 percent of cases have been reported to occur following vaccinations, including hepatitis B vaccination.6,9 Our patient received an influenza vaccination before the onset of brachial plexus neuritis. Some evidence suggests that acute brachial plexus neuritis may be an immunologic disease.10
Most cases of acute brachial plexus neuritis occur between 20 and 60 years of age; however, cases have been reported in all age groups. A male predominance is reported, with a male-to-female ratio ranging from 2:1 to 11.5:1.3,4,11 The annual incidence has been estimated as 1.64 cases per 100,000 persons, but this figure is probably low because many cases may be misdiagnosed, or the symptoms are mild and clinically unrecognized.12 It is not uncommon for patients to present with bilateral acute brachial plexus with only one side being symptomatic.13
Clinical Presentation
The hallmark clinical presentation of patients with acute brachial plexus neuritis is severe, acute, burning pain in the shoulder and upper arm with no apparent cause. On occasion, it may awaken the patient from sleep.1,2,4 In the majority of patients, the pain subsides over the ensuing days to weeks, resulting in a subsequent weakness in the upper arm—at times to the point of muscle flaccidity.2,3,11 This temporal profile of initial arm and shoulder pain followed by muscle weakness as the pain subsides is an important characteristic of acute brachial plexus neuritis.
The usual abnormality evident on physical examination is one of a brachial plexus lesion, as indicated by involvement of two or more nerves14 (Figure 1). Weakness commonly occurs in the supraspinatus, infraspinatus, deltoid and/or the biceps muscles usually involving the upper plexus. However, isolated or single nerve involvement has been clinically reported.15 The course of the neuritis is usually one of gradual improvement and recovery of muscle strength in three to four months.2 Some patients, however, experience several years of muscle weakness or a slight permanent weakness. In general, a longer duration of pain will result in a longer delay in recovering strength.13
FIGURE 1.
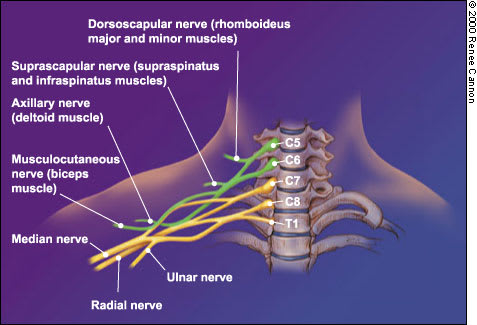
Acute brachial plexus neuritis usually involves the upper plexus, which supplies the shoulder and upper arm muscles. Weakness is frequently found in the rhomboideus major and minor muscles (dorsoscapular nerve), supraspinatus and infraspinatus muscles (suprascapular nerve), deltoid muscle (axillary nerve) and biceps muscle (musculocutaneous nerve).
Differential Diagnosis
Patients with cervical radiculopathy present with pain beginning in the neck area and radiating down the arm for variable distances. The pain may occur after a documented trauma but, not uncommonly, patients may awake in the morning with the pain and no obvious preceding etiology. The pain is associated with partial weakness in the muscles supplied by the involved nerve root and sensory loss in the appropriate dermatome (Tables 1 and 2).
Unlike acute brachial plexus neuritis, the pain, weakness and sensory loss associated with cervical radiculopathy tend to occur simultaneously. While acute brachial plexus neuritis involves multiple nerves of the brachial plexus, a radiculopathy by definition is restricted to one nerve root.
TABLE 1 Comparison of Acute Brachial Plexus Neuritis and Cervical Radiculopathy
| Condition | History | Examination | Tests and results | Treatment |
|---|---|---|---|---|
| Acute brachial plexus neuritis | Intense, burning pain begins in shoulder and upper arm. Pain is unaltered by neck or arm movements. Pain is spontaneous, often with no apparent cause. Gradual decrease in pain followed by marked weakness of upper arm. | Neurologic deficits indicate that more than one nerve is involved (i.e., lesion in the plexus). | Electromyography and nerve conduction studies obtained three to four weeks after symptom onset reveal abnormalities consistent with a brachial plexus lesion. MRI scan of the clinically weak muscles may reveal high signal intensity on T2 images; these changes may appear within days following onset of symptoms. | Analgesics as needed for pain Physical therapy to maintain strength and mobility If deltoid muscle is profoundly weak, recommend a sling to avoid subluxation of humerus. Encourage patient that condition usually, but slowly, improves. |
| Cervical radiculopathy | Pain begins in neck and radiates down the arm for variable distances. Pain is aggravated by neck movements. Pain may begin spontaneously following physical exertion or trauma, but may have no apparent cause. Pain and muscle weakness occur simultaneously. | Weakness and numbness in the distribution of a single nerve root (contemporaneous with the neck and arm pain) | Cervical spine radiograph may reveal interspace narrowing and osteophytes. MRI scan or myelogram followed by computed tomographic scan may reveal osteophyte or herniated disc pulposus consistent with clinical findings. | Analgesics as needed for pain Steroid therapy may help decrease nerve root irritation. Muscle relaxants for muscle spasms Physical therapy Massage and cervical traction Anterior and posterior surgical procedures to decompress involved nerve roots |
MRI = magnetic resonance imaging.
TABLE 2 Cervical Radiculopathy Patterns
| Nerve root involvement | Muscle involvement | Sensory area | Reflex |
|---|---|---|---|
| C5 | Deltoid (shoulder abduction) | Cap of shoulder | None |
| C6 | Biceps (elbow flexion) | Thumb and index finger | Biceps |
| C7 | Triceps (elbow extension) | Middle finger | Triceps |
Diagnostic Evaluation
MRI
In many ways, the use of MRI has improved neuroradiologic evaluation of diverse conditions, including those that involve the peripheral nervous system. In patients with acute brachial plexus neuritis, MRI of the clinically weak muscles may reveal high signal intensity of the affected muscles on the T2 study.2 These changes may appear within days following the onset of symptoms and persist for months. A delayed MRI scan may also reveal muscle atrophy.2 An MRI scan of the plexus and muscles of the shoulder girdle or upper arm is seldom required to establish a diagnosis, but it may be useful if an early, specific diagnosis would be beneficial.
With a typical presentation and an examination suggesting nerve root involvement, the diagnosis of cervical radiculopathy may be confirmed by a myelogram followed immediately by a cervical CT scan. More commonly, however, patients undergo an MRI scan of the cervical spine.
ELECTROMYOGRAPHY
Electromyographic testing in patients with acute brachial plexus neuritis yields variable data, depending on the severity of neural damage and the timing of the examination. It localizes the lesion to the brachial plexus (usually involving the upper aspect of the plexus), and physicians often use results of this test along with a patient history and physical examination to establish the diagnosis. In most cases, three weeks following the onset of paresis, a needle electrode examination will reveal fibrillation potentials and positive waves suggestive of muscle denervation.1 Nerve conduction studies of the medial and ulnar nerves are generally within normal limits. Patients will often recover strength in the denervated muscles approximately three to four months following the initial presentation. This period is characterized by giant polyphasic potentials.1
Treatment
Treatment of patients with acute brachial plexus neuritis includes analgesics, often narcotics (e.g., hydrocodone), which may be required for several weeks, physical therapy for three to eight weeks to help maintain strength and mobility, and encouragement that the condition will slowly improve in the vast majority of patients. The profound weakness in the shoulder muscles may require the use of a sling. Corticosteroids, although frequently used, are not of proven benefit.
Final Comment
Differentiation of acute brachial plexus neuritis from cervical radiculopathy may be problematic in some patients, but it usually is apparent by conducting a careful patient history and performing a neurologic examination. This will separate the single nerve root finding in cervical radiculopathy from the “multiple nerve” findings of a brachial plexus lesion.
Findings on cervical MRI may be helpful if the study is normal or if there is evidence of appropriate nerve root compression, indicating cervical radiculopathy. Difficulty occurs when there are changes of spondylosis at multiple levels because one may be lulled into thinking these radiographic abnormalities account for the clinical deficits. Electromyography and nerve conduction studies are useful, especially when combined with a patient history and physical examination findings, but characteristic changes of a plexus abnormality may not be apparent for three weeks following the onset of symptoms. Differentiating acute brachial plexus neuritis from other diagnoses is important so that surgical treatment is not performed for small osteophytes that may be present on MRI, but are not causing the patient's neurologic deficits.
