
A more recent article on acute otitis externa is available.
Am Fam Physician. 2001;63(5):927-937
See patient information handout on otitis externa, written by the author of this article.
Otitis externa is most commonly caused by infection (usually bacterial, although occasionally fungal), but it may also be associated with a variety of noninfectious systemic or local dermatologic processes. The most characteristic symptom is discomfort that is limited to the external auditory canal, while the most characteristic signs are erythema and swelling of the canal with variable discharge. Excessive moisture and trauma, both of which impair the canal's natural defenses, are the two most common precipitants of otitis externa, and avoidance of these precipitants is the cornerstone of prevention. Thorough cleansing of the canal is essential for diagnosis and treatment, but flushing should be avoided. Acidification with a topical solution of 2 percent acetic acid combined with hydrocortisone for inflammation is effective treatment in most cases and, when used after exposure to moisture, is an excellent prophylactic. Other prophylactic measures such as drying the ears with a hair dryer and avoiding manipulation of the external auditory canal may help prevent recurrence.
Otitis externa is an inflammatory process of the external auditory canal. In one recent study,1 otitis externa was found to be disabling enough to cause 36 percent of patients to interrupt their daily activities for a median duration of four days, with 21 percent requiring bed rest. It is typically a localized process that can be easily controlled with topical agents, yet physicians use systemic medications to treat this condition 65 percent of the time.2 If otitis externa is not optimally treated, especially in immunocompromised patients, the potentially life-threatening infection can spread to the surrounding tissues.
Anatomy and Physiology of the External Auditory Canal
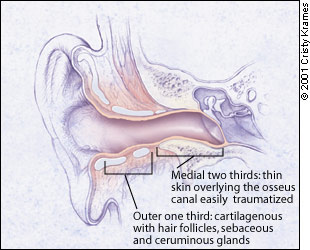
The unique structure of the external auditory canal contributes to the development of otitis externa (Figure 1). It is the only skin-lined cul-de-sac in the human body. The external auditory canal is warm, dark and prone to becoming moist, making it an excellent environment for bacterial and fungal growth. The skin is very thin and the lateral third overlies cartilage, while the rest has a base of bone. The canal is easily traumatized. The exit of debris, secretions and foreign bodies is impeded by a curve at the junction of the cartilage and bone. The presence of hair, especially the thicker hair common in older men, can be a further impediment.
Fortunately, the external auditory canal has some special defenses. Cerumen creates an acidic coat containing lysozymes and other substances that probably inhibit bacterial and fungal growth. The lipid-rich cerumen is also hydrophobic and prevents water from penetrating to the skin and causing maceration. Too little cerumen can predispose the ear canal to infection, but cerumen that is excessive or too viscous can lead to obstruction, retention of water and debris, and infection. Additionally, the canal is defended by a unique epithelial migration that occurs from the tympanic membrane outward, carrying any debris with it.3–5
When these defenses fail or when the epithelium of the external auditory canal is damaged, otitis externa results. There are many precipitants of this infection (Table 1), but the most common is excessive moisture that elevates the pH and removes the cerumen. Once the protective cerumen is removed, keratin debris absorbs the water, which creates a nourishing medium for bacterial growth.
| Moisture | |
| Swimming | |
| Perspiration | |
| High humidity | |
| Water contaminated with bacteria* | |
| High environmental temperatures | |
| Mechanical removal of cerumen | |
| Insertion of foreign objects | |
| Cotton swabs | |
| Fingernails | |
| Hearing aids | |
| Ear plugs | |
| Other trauma to ear canal | |
| Chronic dermatologic disease | |
| Eczema | |
| Psoriasis | |
| Seborrheic dermatitis | |
| Acne | |
Presentation and Evaluation of Otitis Externa
The two most characteristic presenting symptoms of otitis externa are otalgia (ear discomfort) and otorrhea (discharge in or coming from the external auditory canal).2 The ear discomfort can range from pruritus to severe pain that is exacerbated by motion of the ear, including chewing. If inflammation causes sufficient swelling to occlude the external auditory canal, the patient may also complain of aural fullness and loss of hearing.6–8 Otorrhea is also quite variable. Its characteristics often may give a clue to its etiology (Table 2).4,6,9–11
| Cause | Characteristics | |
|---|---|---|
| Otitis externa | ||
| Acute bacterial | Scant white mucus, but occasionally thick | |
| Chronic bacterial | Bloody discharge, especially in the presence of granulation tissue | |
| Fungal | Typically fluffy and white to off-white discharge, but may be black, gray, bluish-green or yellow; small black or white conidiophores on white hyphae associated with Aspergillus | |
| Otitis media with perforated tympanic membrane | ||
| Acute | Purulent white to yellow mucus with deep pain | |
| Serous | Clear mucus, especially in the presence of allergies | |
| Chronic | Intermittent purulent mucus without pain | |
| Cerebrospinal fluid leak | Clear, thin and watery discharge | |
| Trauma | Bloody mucus | |
| Osteomyelitis | Otorrhea with odor | |
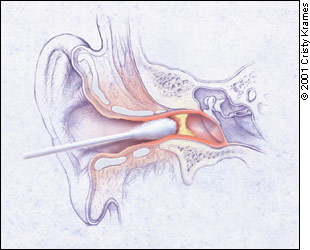
Otorrhea and other debris can occlude the ear canal. Such occlusion makes it difficult to visualize the tympanic membrane and exclude otitis media; it also keeps the canal moist and interferes with topical treatment. It is imperative that this material be removed. However, inflammation makes the external auditory canal even more vulnerable to trauma than usual, and therefore the use of a cerumen spoon or curette should be avoided. Cleansing is best done by suctioning under direct visualization, using the open or operating otoscope head and a 5 or 7 Fr Frazier malleable suction tip attached to low suction. Alternatively, a cotton swab with the cotton fluffed out can be used to gently mop out thin secretions from the external auditory canal, again under direct visualization (Figure 2).
Unless the tympanic membrane can be fully observed and is found to be intact, flushing of the ear canal should not be attempted. A small perforation is often missed, and a tympanic membrane already weakened by infection can easily be disrupted. Divers, surfers and others who experience forceful compression of the tympanic membrane are particularly susceptible to perforations.5,12 Flushing the ear when the tympanic membrane is perforated can disrupt the ossicles and cause significant cochlear-vestibular damage, resulting in hearing loss, tinnitus, vertigo and dizziness. Such damage may necessitate surgery, and a perforated tympanic membrane associated with flushing is a common cause of litigation.13,14 In addition, flushing may cause further trauma to the ear canal.
If the external auditory canal cannot be easily cleansed because of swelling or pain, discharge and debris should be left in place and the patient should undergo frequent reevaluation until the secretions can be removed or have drained spontaneously. When the canal is quite swollen, a cotton wick specifically designed for this purpose should be placed to facilitate drainage and permit application of topical medications.6,10
A thorough examination of the head and neck should be performed to rule out other diagnoses and to look for possible complications of otitis externa. The examination should include evaluation of the sinuses, nose, mastoids, temporomandibular joints, mouth, pharynx and neck. In addition, if the tympanic membrane can be visualized and is red, a pneumatoscope or tympanometry should be used to ascertain whether associated otitis media is present.
Etiology of Otitis Externa
The most common cause of otitis externa is a bacterial infection, although fungal overgrowth is a principal cause in 10 percent of cases.4 Otitis externa can also result from any of a broad range of noninfectious dermatologic processes.
BACTERIAL OTITIS EXTERNA
Etiology and Presentation
The signs and symptoms of otitis externa with a bacterial etiology tend to be more intense than in other forms of the disease. Otalgia may be severe enough to require systemic analgesics such as codeine and non-steroidal anti-inflammatory drugs (NSAIDs).6 Significant swelling of the canal is common. Fever may be present, but if it exceeds 38.3°C (101.0°F), more than simple local otitis externa should be considered. Lymphadenopathy just anterior to the tragus is common.
Topical Treatment
Once the external auditory canal has been cleansed as much as possible and a wick inserted if swelling is severe, topical antibacterial therapy should be started. Because topical agents can be placed in direct contact with the bacteria, simple acidification with 2 percent acetic acid is usually effective, but a wide spectrum of other agents is available (Tables 3 and 4).5,10,12,17–20
| Agent | Cost* | |
|---|---|---|
| 2% Acetic acid otic solution (VoSoL) | $49 (generic: 3 to 10) | |
| With hydrocortisone (VoSoL HC Otic) | 59 (generic: 6 to 12) | |
| With aluminum acetate (Otic Domeboro) | 18 (generic: 7) | |
| Neomycin otic solutions and suspensions | ||
| With polymyxin B–hydrocortisone (Cortisporin) | 42 (generic: 28) | |
| With hydrocortisone-thonzonium (Coly-Mycin S) | 25 (N/A) | |
| Polymyxin B–hydrocortisone (Otobiotic) | 22 (N/A) | |
| Quinolone otic products | ||
| Ofloxacin 0.3% solution (Floxin Otic) | 34 (N/A) | |
| Ciprofloxacin 0.3% and hydrocortisone suspension (Cipro HC Otic) | 59 (N/A) | |
| Quinolone ophthalmic solutions | ||
| Ofloxacin 0.3% (Ocuflox) | 29 (N/A) | |
| Ciprofloxacin 0.3% (Ciloxan) | 30 (N/A) | |
| Aminoglycoside ophthalmic solutions | ||
| Gentamicin sulfate 0.3% (Garamycin) | 19 (generic: 6 to 7) | |
| Tobramycin sulfate 0.3% (Tobrex) | 29 (generic: 13 to 16) | |
| Class | Advantages | Disadvantages |
|---|---|---|
| 2% acetic acid solution | Generic product is inexpensive and effective against most infections without causing sensitization | Can be irritating to inflamed external auditory canal; possibly ototoxic |
| Neomycin otic preparations | Effective, and generic product is inexpensive | Can be a potent sensitizer, causing contact dermatitis in 15% of patients; ototoxic |
| Polymyxin B alone | Avoids potential neomycin sensitization | No activity against Staphylococcus and other gram-positive microorganisms |
| Aminoglycoside ophthalmic solutions | Less locally irritating than 2% acetic acid solution, neomycin otic preparations or polymyxin B alone | Potential ototoxicity; moderately expensive |
| Quinolone otic and ophthalmic solutions | Highly effective without causing local irritation or sensitization; no risk of ototoxicity; twice-daily dosing | Expensive; increased community exposure of an important class of antibiotics, with potential for causing resistance |
Treatment recommendations vary somewhat, but it is most commonly recommended that drops be given for three days beyond the cessation of symptoms (typically five to seven days); however, in patients with more severe infections, 10 to 14 days of treatment may be required. There is no need for reevaluation unless the infection is not resolving.15 Usually, three to four drops are placed in the affected ear four times daily; fluoroquinolone agents, however, are applied twice daily.17,19,20 Warming the bottle of drops in the hands before instillation minimizes dizziness. A small cotton plug moistened with the drops can be used to help retain the drops in the ear if the patient cannot lie still long enough to allow absorption. Absorption may also be facilitated by manipulating the tragus to help distribute the drops throughout the external auditory canal.
When a wick is required, drops should be applied every three to four hours while the patient is awake. In these cases, the ear canal should be reexamined and cleansed every two to five days until edema of the canal has resolved and the wick is no longer needed.6
Systemic Treatment
Oral antibiotics are rarely needed2 but should be used when otitis externa is persistent, when associated otitis media may be present or when local or systemic spread has occurred. The latter should be suspected if the patient's temperature is higher than 38.3°C (101.0°F), if initial pain is severe or if regional lymphadenopathy of the preauricular or anterior or posterior cervical chains is present. Otitis media should be considered when the patient has had an upper respiratory infection or is younger than two years, an age when otitis externa is uncommon. Systemic antibiotics also should be considered when the patient has even early signs of necrotizing otitis externa, as described later. Finally, consideration also should be given to starting oral antibiotics early in patients whose immunity may be compromised, such as those with diabetes, those taking systemic corticosteroids or those with an underlying chronic dermatitis.5,17,21,22
Because ofloxacin otic solution (Floxin Otic) is the only topical agent to be labeled by the U.S. Food and Drug Administration (FDA) for use when the tympanic membrane is perforated,19 oral antibiotics have traditionally been used in this situation. However, because the risk of cochlear damage with the use of other topical medications seems quite small, perforation alone is not an indication for oral antibiotics.6,9,17
When a patient is in a toxic state or the infection is unresponsive to treatment with oral antibiotics, especially in the presence of severe pain and granulation tissue in the ear canal, parenteral antibiotics should be used. Although topical cultures may be misleading, they are recommended by some authors6 to help guide treatment in such severe infections. Patients who do not respond rapidly to parenteral therapy should be referred to an otolaryngologist.
Whether oral or parenteral, empiric treatment should cover Pseudomonas and Staphylococcus species. This would include agents such as the cephalosporins, penicillinase-resistant penicillins and fluoroquinolones.6 Although not labeled by the FDA for pediatric use, fluoroquinolones seem to be safe in children.17 Previous concerns about joint toxicity seem to be unfounded or, at least, cases are extremely rare.23
Complications of Bacterial Otitis Externa
Necrotizing or malignant otitis externa is a life-threatening extension of external otitis into the mastoid or temporal bone. Most commonly caused by P. aeruginosa, it is an osteomyelitis that occurs most often in elderly patients with diabetes mellitus. However, all immunocompromised patients, especially those with human immunodeficiency virus (HIV) infection, are at risk.4,7,17,24
Necrotizing otitis externa is difficult to treat, and the mortality rate can be as high as 53 percent. This condition should be suspected when, despite adequate topical treatment, otalgia and headache are disproportionately more severe than the clinical signs or when granulation tissue is apparent at the bony cartilaginous junction. The diagnosis should be confirmed by a computed tomographic (CT) scan or magnetic resonance imaging (MRI). A combination of technetium scanning to detect osteoblastic activity and gallium 67 imaging to detect granulocytic activity can be used in questionable cases and is recommended by some4,25 as a means of monitoring response to treatment. The erythrocyte sedimentation rate (ESR) can also be used to monitor therapeutic response.25
The excellent antipseudomonal activity of the fluoroquinolones has generally made them the treatment of choice for necrotizing otitis externa, although a combination of a beta-lactam antibiotic and aminoglycoside is also effective.26 In severe cases, a prolonged course of parenteral antibiotics may be needed, but the excellent gastrointestinal absorption of the fluoroquinolones allows milder infections to be treated with a two-week course of oral therapy. Treatment should also include surgical debridement of any granulation or osteitic bone.4,7,25 Thus, an otolaryngologist should usually be involved early in the course, especially if the patient does not respond quickly to appropriate treatment.
Another potential complication of otitis externa is a focal furuncle of the lateral third of the external auditory canal, which can occur as a result of obstructed apopilosebaceous glands. Localized swelling is usually significant and may include a superficial abscess that can be drained. Treatment consists of local heat and topical and systemic antibiotics to eradicate the most common pathogen, S. aureus.4,6
Otitis externa may develop into a persistent low-grade infection and inflammation. In these cases, the external auditory canal lacks cerumen and is lined by dry, hypertrophic skin with variable swelling and stenosis. Mucopurulent otorrhea and excoriated skin may also be present. The causative bacteria vary greatly because many of the patients have already received prolonged topical therapy. At times, only normal flora can be cultured. Treatment consists of the use of acidifying drops combined with steroid drops, but persistent cases require referral to an otolaryngologist for frequent otomicroscopic cleansing and debridement. Rarely, surgery is needed to enlarge and resurface the external auditory canal.4,6
FUNGAL OTITIS EXTERNA
Etiology and Presentation
Fungi are identified in about 10 percent of cases of otitis externa.4,6,16 The most common pathogen is Aspergillus (80 to 90 percent of cases), followed by Candida. Classically, fungal infection is the result of prolonged treatment of bacterial otitis externa that alters the flora of the ear canal. Mixed bacterial and fungal infections are thus common.10,11 However, fungus is occasionally the primary pathogen in otitis externa, especially in the presence of excessive moisture or heat.
The infection is often asymptomatic, and the diagnosis is made by observing the unique discharge in the external auditory canal (Table 2). When symptoms are present, discomfort is again the most common complaint, but in fungal otitis externa this primarily takes the form of pruritus and a feeling of fullness in the ear. The pruritus may be quite intense, resulting in scratching and further damage to the epidermis. Discharge and tinnitus are also common.4,6,10,11
Treatment
Cleansing of the ear canal by suctioning is a principal treatment. Acidifying drops, given three or four times daily for five to seven days, are usually adequate to complete treatment.
Because the infection can persist asymptomatically, the patient should be reevaluated at the end of the course of treatment. At this time any further cleansing can be performed as needed. If the infection is not resolving, over-the-counter clotrimazole 1 percent solution (Lotrimin), which also has some antibacterial activity, can be used. In vitro studies show that topical solutions of thimerosal (Merthiolate) and M-cresyl acetate (Cresylate) are more effective agents but are messier.11 If the tympanic membrane is perforated, tolnaftate 1 percent solution (Tinactin) should be used in order to prevent ototoxicity.11 All of these topical agents are typically used at a dosage of three or four drops twice daily for seven days. Aspergillus infections may be resistant to clotrimazole and may require the use of oral itraconazole (Sporanox).6
Noninfectious Dermatologic Causes of Otitis Externa
Primary dermatologic disorders are frequent precipitants of infectious otitis externa, but they can also be the sole cause of otitis externa. The external auditory canal can be affected by systemic and local dermatologic conditions, often grouped under the term “eczematous otitis externa.”
SYSTEMIC DISEASE
Systemic diseases that may cause otitis externa include atopic dermatitis, psoriasis, seborrheic dermatitis, acne and lupus erythematosus. Lesions typically occur in the external auditory canal and elsewhere on the body, especially the head and neck. There is often a family history and a recurrent course. A thorough dermatologic examination and history should always be part of the evaluation of patients with otitis externa. Manifestations in the external auditory canal can range from mild erythema and scaling with atopic dermatitis, to dense, adherent scaling with psoriasis, to the focal inflammatory changes of acne. Pruritus is the most common symptom.
Control of the disease elsewhere will reduce the manifestations in the ear canal and is therefore the cornerstone of treatment. In addition, otitis from all of these diseases, excluding acne, will respond to low-dose therapy with topical steroid solutions. Steroids, however, can lead to bacterial or fungal overgrowth in patients with already compromised skin. Thus, an acidifying agent is often added. Acne will often respond to topical benzoyl peroxide lotions and antibiotic solutions. Seborrheic dermatitis of the external ear can be treated with medicated shampoo used for the scalp. Difficult cases should be referred to a dermatologist.6,10,27
LOCAL DISEASE
Contact dermatitis, irritant or allergic, can involve the pinna as well as the external auditory canal. Allergic forms usually present acutely with erythematous, pruritic, edematous and exudative lesions, while contact dermatitis often has a more insidious onset with lichenification. Both types can be complicated by secondary bacterial infections. Contact dermatitis in the ear canal can result from almost any local irritant, including topical anti-infective agents and anesthetics and other topical preparations. It also may be associated with the use of hearing aids and ear plugs. Hypoallergenic silicone hearing aids are now available.
The most important treatment is identifying and removing the irritant or allergen. Topical steroids are beneficial, including a cream for the pinna when it is involved. An acidifying agent, usually Burow's otic solution with 2 percent acetic acid (Otic Domeboro), is often added to prevent secondary infections, reacidify the skin, dry weeping lesions and remove crusts. Three to five days of use, three or four times daily, is usually sufficient for topical therapy. Systemic steroids and antihistamines may be needed for severe allergic reactions.4,6,10,27
Clinical characteristics helpful in differentiating the noninfectious causes of otitis externa are summarized in Table 5.
| Disease | Clinical characteristics |
|---|---|
| Atopic dermatitis | Chronic, intensely pruritic reaction to allergens or stress |
| Poorly circumscribed erythema and small papules, often obscured by excoriation associated with pruritus | |
| Excoriation may cause lichenified and hyperpigmented external auditory canal over time | |
| Typically part of more generalized skin involvement, including the external ears, face and neck | |
| Commonly associated with personal or family history of atopy of the respiratory tract or eyes | |
| Typical onset in childhood | |
| Psoriasis | Idiopathic, chronic, inflammatory, proliferative skin disease |
| Commonly associated with scalp involvement but rarely with facial involvement | |
| Raised, red lesions with thick, silvery-white adherent scale | |
| Often pruritic | |
| Seborrheic dermatitis | Powdery or greasy scale with pink or orange base; typically not as thick as in psoriasis |
| Typically associated with scalp, face, upper trunk involvement | |
| Often associated with parkinsonism, Down syndrome and other neurologic conditions; may be associated with HIV infection | |
| Acne | Closed and open comedones with occasional pustules; similar findings on face and upper trunk |
| Lupus erythematosus | Multisystem autoimmune disease; look for other organ involvement when present |
| Ear canal involvement commonly associated with discoid form of the disease; epidermal atrophy causes shiny surface and telangiectasia | |
| Usually associated with erythema and scaling with hypopigmentation | |
| Contact dermatitis due to irritant | Dose-dependent response to irritants ranging from acids to alkalis to excess water |
| Insidious onset with lichenification | |
| Allergic contact dermatitis | Less dose-dependent than irritant contact dermatitis; requires predisposition to react to the allergen |
| External auditory canal may react to allergens that do not cause a reaction elsewhere | |
| Erythema, pruritus, edema and exudate with occasional vesiculation |
Prevention of Recurrence
Prevention of recurrence of otitis externa primarily consists of avoiding the many precipitants that have been discussed and treating any underlying chronic dermatologic disorders. This is particularly important for patients with unusually viscous cerumen, a narrowed external auditory canal or systemic allergies,5 especially in those who are immunosuppressed. Prevention is also important in patients who perspire excessively or participate in water sports regularly.
After bathing or swimming, the external auditory canal should be dried using a hair dryer on the lowest heat setting. Acidifying drops can then be instilled. Some authors4,9 recommend combining the acidifying agent with alcohol drops (Swim Ear) to act as an astringent, but many physicians feel this is too irritating and prefer using Burow's solution as the astringent (Star-Otic). Obviously, any manipulation of the skin of the external auditory canal (such as scratching or overzealous cleaning) should be avoided.6
Any time the external auditory canal is cleaned and cerumen is removed, the canal becomes more vulnerable to infection. Therefore, if there has been any trauma, and especially if syringing has left the external auditory canal wet, use of an acidifying agent with hydrocortisone is a good prophylactic measure.4,12 If the cerumen is difficult to remove, a ceruminolytic agent such as Cerumenex or even a simple 4 percent baking soda solution should be used in the office to soften the cerumen first to avoid traumatizing the external auditory canal.9
Persons who swim frequently should use a barrier to protect their ears from water. However, impermeable ear plugs act as a local irritant and have been shown to predispose the ear canal to otitis externa. A tight-fitting bathing cap offers better protection.5,28 Patients with acute otitis externa should preferably abstain from water sports for at least seven to 10 days,28 although some authors would allow competitive swimmers to return after two or three days of treatment as long as all pain has resolved.12 Others would allow return with the use of well-fitting ear plugs.5
Although otitis externa has a variety of causes, there are some unifying principles of evaluation and treatment that allow expeditious management of most cases (Table 6). However, otitis externa is a disease process that should be treated aggressively because it can cause significant morbidity and even life-threatening complications.
| Discomfort limited to the external auditory canal is the most characteristic symptom. | |
| Thorough cleansing of the external auditory canal whenever possible is essential for diagnosis and treatment, but flushing should be avoided. | |
| Look for signs and symptoms indicating that the process extends beyond the external auditory canal, including: | |
| Evidence of associated otitis media on otoscopic examination. | |
| Severe pain or granulation of the external auditory canal in patients with diabetes or those who are immunocompromised | |
| Evidence of an underlying systemic dermatologic process. | |
| Avoid moisture and trauma in the external auditory canal to prevent recurrence. | |
| Acidification with 2 percent acetic acid combined with hydrocortisone (VoSoL HC Otic) for inflammation is effective treatment in most cases and, when used after exposure to moisture, is an excellent prophylactic. | |