
Am Fam Physician. 2002;65(1):105-106
A 65-year-old male with a 94 pack-year history of smoking presented with a draining, swollen thumb (Figure 1). The patient recalled no specific history of trauma, but had been engaged in the harvesting of crops. On examination, the thumb was noted to be markedly erythematous, indurated, and warm. Areas of fluctuance could be palpated, but the patient had no other symptoms. Plain radiographs of the thumb revealed near-complete destruction of the distal phalanx (Figure 2).


Question
Discussion
The answer is D: metastatic carcinoma. Carcinoma metastatic to the hand is rare. Large swelling that produces little pain is typically found in the history. In addition, swelling that takes place over the course of several weeks, rather than days, is suspicious for a tumor.1 Metastatic lesions may be confused with a ganglion, epidermoid inclusion cyst, acute gout, and even rheumatoid arthritis.
Metastatic carcinoma initially is similar to a paronychia, which may lead to a delay in diagnosis. Radiographs showing bony destruction may lead to the conclusion that the lesion, which appears to be a pulp space infection, has caused a secondary osteomyelitis. Metastatic lesions to the nail bed tend to lift up the nail, exposing the underlying tissues to trauma and secondary infection.2
Radiographs of phalangeal metastasis commonly demonstrate an osteolytic lesion and a lack of periosteal reaction. In addition, they usually do not penetrate the joint space. Even with extensive destruction, a thin margin of periarticular bone is characteristically preserved.2
The most common source of metastasis to the hand is primary bronchogenic carcinoma. Other cancers that metastasize to bone include carcinomas of the kidney, prostate, colon, and breast. A review3 published in 1983 showed that of 156 cases of metastatic lesions to the hand, 52 were from lung tumors and 15 were from breast cancer. Occasionally, a phalangeal metastasis may be the first manifestation of a bronchogenic carcinoma.
Because of the poor prognosis associated with widely metastatic disease, therapy is usually directed at palliation of symptoms.4 This may require disarticulation, amputation, and radiation therapy.
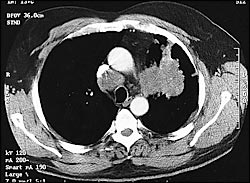
In this patient, chest radiographs revealed a mass in the left lung measuring 9 cm × 7 cm. Computed tomographic (CT) scanning of the chest showed extension to the surrounding ribs and biopsy revealed nonsmall-cell carcinoma (Figure 3). A CT scan of the head and abdomen revealed metastasis to the brain and lumbar vertebral bodies. Treatment for this patient has included thumb amputation and palliative radiotherapy to the brain, right hand, mediastinum, and lumbar spine.
In contrast to rare metastatic lesions, paronychial infections are seen commonly by primary care physicians. A paronychia is an infection of the soft tissues along the side of the fingernail plate. Often, it is the result minor trauma, such as nail biting, puncture wound, hangnail, or foreign body. An eponychia is an infection at the proximal nail and cuticle. Often, it is the result of a paronychia that extends proximally.5 In early stages, paronychial and eponychial infections can be treated with warm soaks, elevation, and oral antibiotics. Empiric antibiotic therapy should cover Staphylococcus aureus. Anaerobic coverage also may be needed if there is the possibility of oral contamination. Both entities can progress to an abscess, which requires incision and drainage.
Although melanoma can appear under the nail, it would not tend to involve the bone at such an early stage. The same is true for a squamous cell carcinoma of the skin. Sporotrichosis is a deep-seated fungal injection, usually found in the lower extremities, but likewise does not cause such early bone destruction.