
Am Fam Physician. 2002;65(6):1155-1158
A patient information handout on punch biopsy of the skin is provided on page 1167.
Skin biopsy is one of the most important diagnostic tests for skin disorders. Punch biopsy is considered the primary technique for obtaining diagnostic full-thickness skin specimens. It requires basic general surgical and suture-tying skills and is easy to learn. The technique involves the use of a circular blade that is rotated down through the epidermis and dermis, and into the subcutaneous fat, yielding a 3- to 4-mm cylindrical core of tissue sample. Stretching the skin perpendicular to the lines of least skin tension before incision results in an elliptical-shaped wound, allowing for easier closure by a single suture. Once the specimen is obtained, caution must be used in handling it to avoid crush artifact. Punch biopsies are useful in the work-up of cutaneous neoplasms, pigmented lesions, inflammatory lesions and chronic skin disorders. Properly administered local anesthesia usually makes this a painless procedure.
Skin biopsy is the most important diagnostic test for skin disorders. In selected patients, a properly performed skin biopsy almost always yields useful diagnostic information. Some authors believe that most errors in dermatologic diagnosis occur because of failure to perform a prompt skin biopsy.
Punch biopsy is considered the primary technique to obtain diagnostic, full-thickness skin specimens. It is performed using a circular blade or trephine attached to a pencil-like handle. The instrument is rotated down through the epidermis and dermis, and into the subcutaneous fat. The punch biopsy yields a cylindrical core of tissue that must be gently handled (usually with a needle) to prevent crush artifact at the pathologic evaluation.
Large punch biopsy sites can be closed with a single suture and generally produce only a minimal scar. Because linear closure is performed on the circular-shaped defect, stretching the skin before performing the punch biopsy allows the relaxed skin defect to appear more elliptical and makes it easier to close. The skin is stretched perpendicular to the relaxed skin tension lines, so that the resulting elliptical-shaped wound and closure are parallel to these skin tension lines.
Punch biopsy of inflammatory dermatoses can provide useful information when the differential diagnosis has been narrowed. Cutaneous neoplasms can be evaluated by punch biopsy, and the discovery of malignancy may alter the planned surgical excision procedure. Routine biopsy of skin rashes is not recommended because the commonly reported nonspecific pathology result rarely alters clinical management.
Methods and Materials
EQUIPMENT
Nonsterile Tray for Anesthesia
Place the following items on a nonsterile drape covering a Mayo stand:
Nonsterile gloves
1 inch of 4 × 4 gauze soaked with povidone-iodine solution
3-mL syringe filled with 2 percent lidocaine with epinephrine (Xylocaine with epinephrine) and a 30-gauge needle
Labeled formalin container(s) for the number of biopsies to be performed
Sterile Tray for the Procedure
Place the following items on a sterile drape covering a Mayo stand:
Sterile gloves (Some physicians choose to perform the procedure using the nonsterile gloves that were used to administer the anesthesia.)
Desired punch biopsy instrument (3 or 4 mm)
Needle holder for suturing
Desired size of suture (4–0, 5–0 or 6–0 nylon, depending on body site)
Iris scissors
21-gauge, 1¼-inch needle for elevating the specimen, if a sterile instrument is used (alternatively, the nonsterile anesthesia needle can be used)
Sterile fenestrated drape (Some physicians choose to perform the procedure without a covering drape.)
Procedure Description
The area to be biopsied should be selected. Commonly selected sites are the most abnormal-appearing site within a lesion or the edge of an actively growing lesion.
The skin is cleansed with povidone-iodine solution and anesthetized with 2 percent lidocaine with epinephrine. A 30-gauge needle is used to administer the anesthetic to limit discomfort.
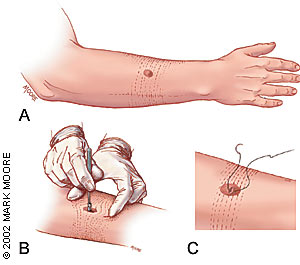
The lines of least skin tension should be identified for the area to be biopsied. For example, on the arm, these lines run perpendicular to the long axis of the extremity. The incision line created by the suturing after the biopsy is performed will be oriented parallel to the lines of least skin tension. Physicians who cannot recall the line orientation for a specific body area should consult the widely published drawings of these lines.
The skin surrounding the biopsy site is stretched with the thumb and index finger of the nondominant hand (Figure 1). The skin is stretched perpendicular to the lines of least skin tension. When the skin relaxes after the biopsy is performed, an elliptical-shaped wound remains that is oriented in the same direction as the lines of least skin tension. On the arm, the skin is stretched along the long axis of the extremity.
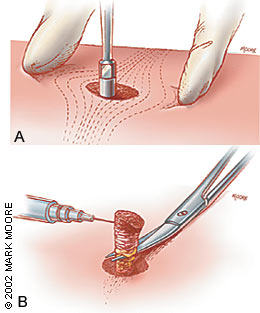
The punch biopsy instrument is held vertically over the skin and rotated downward using a twirling motion created by the first two fingers on the dominant hand (Figure 2). Once the instrument has penetrated the dermis into the subcutaneous fat, or once the instrument reaches the hub, it is removed.
The cylindrical skin specimen is elevated with the anesthesia needle held in the non-dominant hand. The use of forceps is discouraged because these instruments frequently cause crush artifact. Scissors held in the dominant hand cut the specimen free from the subcutaneous tissues. The cut is made below the level of the dermis.
The wound is closed, if necessary, with one or two interrupted nylon sutures: 5–0 nylon is used for most nonfacial areas, and 6–0 nylon for most facial areas. The suture generally creates good hemostasis, and antibiotic ointment and a bandage are then applied.
Follow-Up
Melanoma. Results from a punch biopsy revealing malignancy usually mandate further surgical intervention. If the lesion is a thin melanoma (less than 0.75-mm thick) and the specimen was from an area of average thickness for the lesion, the family physician can perform the excision of the lesion with at least a 5-mm margin of normal surrounding skin. If the lesion is a thicker melanoma, the family physician may consider referral to a melanoma center for excision and sentinel node removal following dye injection.
Other Skin Malignancy. Basal cell carcinoma and squamous cell carcinoma can be completely excised with a 4- to 6-mm margin of normal appearing skin. The larger margin (6 mm) is recommended for larger tumors, recurring tumors or tumors on high-risk sites such as the nose, ears and eyelids. Other, less common tumors, such as dermatosarcoma protuberans, may require referral for more extensive surgical management.
Benign Growths. The follow-up of benign growths depends on the particular lesion, patient preference and cosmetic concerns. Some patients may prefer to leave a benign growth alone. Others may request a fusiform or shave excision. Some benign growths that are premalignant (such as actinic keratoses) can be managed with ablative cryotherapy or peeled off with fluorouracil therapy.
Inflammatory Lesions. The specific cause for an inflammatory skin change should be sought. Further medical testing (e.g., radiographs or blood work) that can be ordered depends on the information provided in the report from the pathologist. For example, an angiotensin-converting enzyme level might be ordered if results of the skin biopsy reveal sarcoidosis. Sometimes the pathologist cannot define the specific inflammatory lesion but can narrow the differential diagnosis to allow for therapeutic intervention.
Chronic Skin Disorders. Chronic papulosquamous disorders or other skin problems can be correctly identified and proper therapy initiated. An example is a patient with an early psoriasis plaque, whose atypical-appearing lesion is correctly identified by punch biopsy.
Procedure Pitfalls/Complications
The Procedure Is Uncomfortable for the Patient. This procedure should rarely be associated with discomfort. Slow and adequate anesthesia infiltration of the area should make this a painless procedure. If the anesthetic is administered subcutaneously, it may take a minute for full anesthetic effect to take place, compared with the almost immediate effect of an intradermal route of administration.
Nerve Injury Develops From the Procedure. Many physicians have been taught to rotate the punch instrument down to the hub. This produces a circular incision that may penetrate up to three-eighths of an inch below the skin surface, depending on the punch instrument that is used. On the areas where the skin is thin, such as the face or dorsum of the hand, it is possible to damage arteries, nerves and veins below the skin. Most physicians can identify when the instrument penetrates the skin, because a “give” can be felt. Once the instrument has penetrated the dermis into the subcutaneous fat, downward pressure should be stopped. The physician should use care when punch biopsy procedures are performed on the face, neck or distal extremities.
It Is Time Consuming to Switch From Non-sterile to Sterile Gloves. Many physicians perform the procedure using the nonsterile gloves that were used to administer the anesthesia. While this means that the suturing is performed with nonsterile gloves, it is highly unusual for infection to develop at a punch biopsy site.
Physician Training
Punch biopsy is a simple technique to learn and perform. Supervision is rarely needed after a physician has performed two or three procedures. General surgical and suture-tying skills are needed when suture closure of the wound is performed.