Joint injection of the elbow is a useful diagnostic and therapeutic tool for the family physician. In this article, the injection procedures for the elbow joint, medial and lateral epicondylitis, and olecranon bursitis are reviewed. Persistent pain related to inflammatory conditions responds well to injection in the region. Indications for elbow joint injection include osteoarthritis and rheumatoid arthritis. Corticosteroid injection is an accepted treatment option for medial and lateral epicondylitis. Olecranon bursa aspiration and injection are useful when that bursa is inflamed. The proper techniques, choice and quantity of pharmaceuticals, and appropriate follow-up essential for effective outcomes are discussed.
This article, another in a series on diagnostic and therapeutic injections, covers the elbow region. The rationale, indications, contraindications, and general approach to this technique are covered in the first article in the series, published in the July 15, 2002, issue of American Family Physician.1
Arthritis of the Elbow Joint
ANATOMY
The elbow joint is formed by three articulations: the humerus with the radius, the humerus with the ulna, and the radius with the ulna. The elbow is a joint that serves to move the distal extremity to position the hand for fine motor activities. Soft tissues, tendons, and ligaments stabilize the bony articulations. The ulnar nerve passes medial to the olecranon process and behind the medial epicondyle in the cubital tunnel.
INDICATIONS
The major indications for elbow joint injection are osteoarthritis, rheumatoid arthritis2 and, to a lesser extent, crystal arthropathies.3 Radial head fractures, resulting from traumatic injury, also can be an indication for aspiration and analgesic injection. To aid in the diagnosis of fracture comminution and possible mechanical blockade, and to provide relief from swelling and pain, the joint can be aspirated and injected with a local anesthetic.4,5 Reduced range of motion despite analgesic injection is diagnostic in such instances. A history of trauma and blood or fat globules in the joint aspirate should raise the possibility of fracture even in the absence of evidence of fracture on radiographs.
TIMING AND OTHER CONSIDERATIONS
Joint injection in this area should be considered only after other appropriate therapeutic interventions have been undertaken. These include the use of acetaminophen, nonsteroidal anti-inflammatory drugs (NSAIDs), other disease-modifying agents for rheumatoid arthritis, and physical therapy.
TECHNIQUE
Pharmaceuticals and equipment are listed in Table 1. The patient should be in a supine position with the elbow flexed to 45 degrees and the hand in a neutral position resting on the patient's thigh.
TABLE 1 Equipment and Pharmaceuticals for Injection of the Elbow Region
| Site | Syringe | Needle | Anesthetic | Corticosteroid* | Hydrocortisone equivalents per injection (mg) | |
|---|---|---|---|---|---|---|
| Elbow joint aspiration | 20 mL | 18 or 22 gauge, 1.5 inch | ||||
| Elbow joint injection† | 5 or 10 mL | 25 gauge, 1 to 1.5 inch | 3 to 5 mL of 1% lidocaine (Xylocaine) or 0.25 or 0.5% bupivacaine (Marcaine) | 1 to 2 mL betamethasone sodium phosphate and acetate (Celestone Soluspan) | 150 to 300 | |
| or | ||||||
| 1 to 2 mL methylprednisolone (Depo-Medrol), 40 mg per mL | 200 to 400 | |||||
| Medial and lateral epicondylitis | 5 mL | 25 gauge, 1 inch | 2 to 3 mL of 1% lidocaine or 0.25 or 0.5% bupivacaine | 1 mL betamethasone sodium phosphate and acetate | 150 | |
| or | ||||||
| 1 mL methylprednisolone, 40 mg per mL | 200 | |||||
| Olecranon bursitis aspiration | 10 to 20 mL | 18 or 22 gauge, 1 inch | ||||
| Olecranon bursitis injection | 5 mL | 25 gauge, 1 inch | 3 mL of 1% lidocaine or 0.25 or 0.5% bupivacaine | 1 mL betamethasone sodium phosphate and acetate | 150 | |
| or | ||||||
| 1 mL methylprednisolone, 40 mg per mL | 200 | |||||
*—Other preparations such as triamcinolone (Aristocort) or dexamethasone may be used.
† —A hemostat is needed to immobilize the needle when performing injection following aspiration. Corticosteroid injection is not performed in suspected or confirmed radial head fractures.
Essential landmarks to palpate before performing this injection are the soft tissue at the center of the triangle formed by the lateral olecranon, the head of the radius, and the lateral epicondyle.
Sterile technique must be followed. The elbow joint is injected from a lateral approach, thereby avoiding the ulnar nerve. The needle is inserted into the soft tissue within the triangle described in the previous paragraph, and directed to the opposite (medial) epicondyle (Figure 1). Aspiration of fluid or the easy flow of injectables suggests that the needle is properly positioned in the joint space. If the needle hits against bone, it should be pulled back and redirected at a slightly different angle. As with any injection, the physician should first aspirate to ensure that the needle is not in a blood vessel. The injection should be made slowly but with consistent pressure.
FIGURE 1.
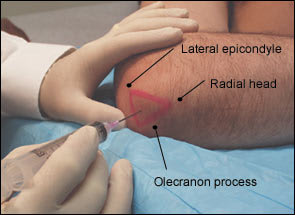
Anatomic triangle for joint injection or aspiration.
FOLLOW-UP
After injection, the joint should be put through passive range of motion to determine if pain relief has been achieved. See Table 2 for other aspects of follow-up care.
TABLE 2 Follow-Up Care After Elbow Injection
| The patient should do the following: |
| Remain in a supine position for one to two minutes. |
| Be monitored for adverse reactions for 30 minutes. |
| Avoid strenuous activity for 48 hours. |
| Treat steroid flare with ice and nonsteroidal anti-inflammatory drugs. |
| Schedule follow-up within three weeks. |
Lateral and Medial Epicondylitis
ANATOMY
The lateral epicondyle is the site of origin of the wrist extensorsupinator muscle group, while the medial epicondyle is the site of origin of the wrist flexor-pronator muscle group. The pathologic process of epicondylitis involves chronic degenerative changes of the tendons (tendinosis) at the region of the respective epicondyles.
INDICATIONS AND DIAGNOSIS
The indication for injection therapy for epicondylitis is usually chronic pain and disability not relieved by more conservative means, or severe acute pain with functional impairment that calls for a more rapid intervention.6–8 A systematic, evidence-based review9 concluded that corticosteroid injections appear to be relatively safe and seem to have a short-term effect (two to six weeks). A more recent, multicenter, randomized controlled trial10 concluded that corticosteroid injections are effective in providing early symptom relief.
Lateral and medial epicondylitis are most often the result of repetitive activities such as golf, racquet or throwing sports, or occupation-related movements such as hammering, hand sanding, lifting, or point-and-click motions from moving a computer mouse. Patients typically present with a history of insidious onset of pain and tenderness of the affected elbow region, and a weakened hand grip. The examination reveals point tenderness in the region of the epicondyle, and pain and weakness exacerbated by resisted wrist extension and supination for lateral epicondylitis, and with resisted wrist flexion and pronation for medial epicondylitis.
TIMING AND OTHER CONSIDERATIONS
Therapeutic injection for epicondylitis should be performed only after a trial of other therapeutic modalities such as use of NSAIDs and avoiding aggravating activities.11 To date, there is no conclusive evidence to show that orthotic devices are effective in treating lateral epicondylitis.12 Immobilization of the elbow should be avoided.
TECHNIQUE
Pharmaceuticals and equipment are listed in Table 1. Patients are placed in the supine position. For lateral epicondylitis, the affected arm should rest at the side with the elbow flexed to 45 degrees and the wrist pronated. For medial epicondylitis, the injection should proceed with the affected arm resting comfortably abducted and the hand supinated.
The most tender point of the epicondyle is identified by gentle palpation. The needle is inserted at 90 degrees down to the level of the bone and then pulled back 1 to 2 mm (Figures 2 and 3). The pharmaceutical solution is injected evenly and slowly.
FIGURE 2.

Medial epicondyle injection site.
FIGURE 3.

Lateral epicondyle injection site.
FOLLOW-UP
After injection, the wrist extensors or flexors are stressed to ascertain proper delivery of the pharmaceutical. See Table 2 for other aspects of follow-up care.
Olecranon Bursitis
ANATOMY
The olecranon bursa is superficial to the olecranon process and extra-articular to the elbow joint.
INDICATIONS AND DIAGNOSIS
Olecranon bursitis commonly occurs after repetitive trauma to the elbow or in patients with rheumatoid or crystalloid arthritis. On physical examination, a swollen, fluid-filled sac is noted and palpated over the olecranon. The swelling is relatively painless. Aspiration of an inflamed bursa can be performed for relief of discomfort associated with bursitis. If the symptoms of olecranon bursitis are recurrent, corticosteroid injection may be performed.
The olecranon bursa may also be the site of infection, frequently caused by Staphylococcus aureus. If an infection is suspected because of the history and a tender, hot bursa with purulent drainage is found on examination, fluid for Gram stain and culture may be obtained by aspiration. Corticosteroids should not be injected if an infected bursa is suspected.
TIMING AND OTHER CONSIDERATIONS
Aspiration of the olecranon bursa may be performed acutely for relief of swelling and discomfort. Corticosteroid injection can be performed in chronic or persistent bursitis after a trial of more conservative therapy.13
TECHNIQUE
Pharmaceuticals and equipment are listed in Table 1. The patient is placed in the supine position with the elbow flexed as much as the patient can comfortably tolerate. Elbow flexion allows for easier aspiration.
The area over the olecranon process is palpated for fluctuance. To perform the injection or aspiration, the needle is inserted directly into the bursa. Fluid is easily aspirated when the needle is properly positioned. When aspirating for culture, sterile technique should be used. If aspirating and injecting, the needle is held in place with a hemostat while the syringe is changed (Figure 4).
FIGURE 4.

Olecranon bursa injection site.
FOLLOW-UP
A pressure dressing should be applied after aspiration and injection. See Table 2 for other aspects of follow-up care.
