The hand can be anesthetized effectively with blocks of the median, ulnar, or radial nerve. Each digit is supplied by four digital nerves, which can be blocked with injections on each side of the digit. Anterior or posterior ankle blocks can be used for regional anesthesia for the foot. The anterior ankle block, which is used for procedures on the dorsum of the foot, involves blocking the saphenous nerve, and superficial and deep peroneal nerves. The posterior ankle block, which is used to anesthetize the sole of the foot, involves blocking the sural and posterior tibial nerves. Paracervical block is used for procedures on the cervix, such as loop electrocauterization or conization. Dorsal penile block has been the most commonly recommended anesthetic technique for neonatal circumcision. A safe and effective alternative is the application of anesthetic cream over the skin to be circumcised.
Familiarity with local anatomic landmarks for each injection is key to obtaining successful regional anesthesia. Part II of this two-part article focuses on nerve blocks of the extremities and perineum.
Median Nerve Block
The median nerve provides sensations to the radial aspect of the palm, palmar surface of the thumb, index finger, middle finger, radial half of the ring finger, and the nail beds of the same digits.1 The nerve enters the hand between the flexor carpi radialis and palmaris longus tendons beneath the flexor retinaculum. Both tendons are identified by asking the patient to oppose the thumb and the fifth digit.2 The needle is angled at 45 degrees and enters between the tendons at the level of the proximal wrist crease. Injecting 2 to 5 mL of local anesthetic will block the median nerve (Figure 1). If the patient has congenital absence of the palmaris longus muscle, the injection can be made on the medial aspect (toward the ulna) of the flexor carpi radialis tendon.3 As the needle passes through the flexor retinaculum, a loss of resistance is felt, marking the point at which the injection should be made. If paresthesias are elicited, the needle should be withdrawn slightly (i.e., approximately 2 mm) to avoid nerve fiber damage or intraneural injection.
Carpal tunnel syndrome has been identified as a relative contraindication to this block,2 although anesthetic and steroid combination commonly is injected at this site for treatment of the syndrome. A superficial palmar branch supplying the skin over the thenar area can be blocked by subcutaneous injection of 0.5 to 1.0 mL of anesthetic solution above the retinaculum.4
FIGURE 1.

Median nerve block.
Radial Nerve Block
The superficial branch of the radial nerve supplies the dorsum of the hand and first three fingers proximal to the distal interphalangeal joint.5 Because it branches extensively before reaching the wrist, a broad area needs to be anesthetized for a complete block to be achieved. First, 3 mL of 1 percent lidocaine (Xylocaine) is injected just lateral to the radial artery at the proximal wrist crease. The needle is then redirected and advanced subcutaneously across the proximal border of the snuffbox toward the middle of the dorsal wrist. Approximately 5 to 7 mL of anesthetic is injected in a cufflike fashion as the needle is withdrawn (Figure 2). Several needle entry sites may be necessary to follow the curve of the radial aspect of the wrist and adequately cover the entire area.
FIGURE 2.

Radial nerve block.
Ulnar Nerve Block
The ulnar nerve divides into palmar and dorsal branches at the proximal flexor crease of the wrist, supplying the ulnar aspect of the palmar and dorsal surface of the hand and fifth finger, and ulnar half of the fourth finger. Injection of 5 to 7 mL of anesthetic 1 to 2 cm deep between the flexor carpi ulnaris tendon and the ulnar artery blocks the palmar branch of the ulnar nerve (Figure 3, part A). The dorsal ulnar branch is blocked by subcutaneous infiltration with 3 to 4 mL of solution distal to the ulnar styloid process (Figure 3, part B).
FIGURE 3.

Ulnar nerve block. (A) Needle placement for blocking the palmar branch of the ulnar nerve. (B) Needle placement for blocking the dorsal ulnar branch.
Both branches of the ulnar nerve also can be blocked at the elbow. With the elbow flexed at 90 degrees, the needle is inserted 0.5 cm into the skin between the olecranon and the medial epicondyle, and 3 to 5 mL of solution is injected.6 The potential for nerve damage is higher with this procedure because the nerve can be trapped between local anesthetic and the bone, causing nerve ischemia.
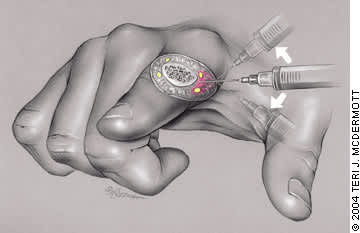
Digital Nerve Block
The two nerves running on each side of the fingers and toes can be blocked with injections on each side of the digit (Figure 4). The needle is inserted down to the bone, midway between the palmar and dorsal surfaces of the digit, 1 to 2 cm distal to the web space. The anesthetic is administered with the needle perpendicular to the digit, then angled slightly topward the palmar and dorsal surfaces as additional solution is injected. Less than 1.5 mL of anesthetic usually is required on each side of the digit.7
A web space block also can be performed. The needle is inserted from the dorsal aspect of the web space and advanced until the tip tents the palmar skin. Anesthetic is administered along the side of the digit as the needle is withdrawn. Care should be taken not to infiltrate circumferentially, which can lead to vascular compromise. Epinephrine should not be used in digital blocks.8
Ankle Blocks
POSTERIOR ANKLE BLOCK
Local anesthesia of the sole of the foot is relatively difficult because of marked tenderness with needle penetration; regional nerve block often is preferred. The posterior ankle block (Figure 5, part A) is used to anesthetize the sole of the foot by blocking the sural and posterior tibial nerves. The sural nerve runs behind the fibula and lateral malleolus, and supplies the heel and lateral aspect of the foot.9 To perform a sural nerve block, the patient is positioned prone with the foot in slight dorsiflexion. The needle is inserted lateral to the Achilles tendon and 1 to 2 cm above the level of the distal tip of the lateral malleolus. The anesthetic is infiltrated as the needle is redirected in a fan-shaped pattern from side to side to ensure adequate coverage of the nerve.
The tibial nerve, located between the medial malleolus and Achilles tendon, supplies the medial portion of the sole and the medial side of the foot.9 The nerve runs next to the posterior tibial artery and is posterior to the pulse. To block the tibial nerve, the patient is positioned prone with the foot in slight dorsiflexion. The needle is inserted anterior to the Achilles tendon 1 to 2 cm above the level of the medial malleolus, and a wheal is placed over the skin. The needle is advanced through the wheal toward the posterior tibial artery. The tibial nerve lies under the dense flexor retinaculum; the give of the needle should be felt as it perforates the retinaculum. Approximately 5 mL of 1 percent lidocaine is injected around the nerve after aspiration to avoid intra-arterial injection. Another 5 mL is injected as the needle is withdrawn.
FIGURE 4.
Digital nerve block.
ANTERIOR ANKLE BLOCK
The anterior ankle block (Figure 5, part B) is used for procedures on the dorsum of the foot and involves anesthesia of the saphenous nerve, and superficial and deep peroneal nerves.10 The deep peroneal nerve supplies the space between the first and second toes; it is located between the anterior tibialis tendon and extensor hallucis longus tendon.
With the patient supine and the ankle in slight plantarflexion, the needle is inserted at the upper level of the malleoli between the tendons of the tibialis anterior and extensor hallucis longus. These tendons can be accentuated by dorsiflexing the ankle and the great toe against resistance.6 If the anterior tibial artery can be palpated, the needle should be inserted just lateral to the artery. The needle is advanced deep to the tendons just above the periosteum, and 5 mL of 1 percent lidocaine is injected after aspiration.
FIGURE 5.
Needle placement for administering ankle blocks. (A) Posterior ankle block. (B) Anterior ankle block.
The superficial peroneal nerve can be blocked by inserting the needle immediately above and anterior to the lateral malleolus. Approximately 5 mL of anesthetic is infiltrated subcutaneously between the anterior border of the tibia and the superior aspect of the lateral malleolus. The saphenous nerve, which runs medial to the great saphenous vein, can be blocked by inserting the needle immediately above and anterior to the medial malleolus and injecting 3 to 4 mL of anesthetic into the subcutaneous tissue around the great saphenous vein.
Paracervical Block
The paracervical block is used for procedures on the cervix (e.g., loop electrocauterization, conization). This block usually is not used in pregnant women because of the potential risk for anesthetic crossing over to the fetal circulation. After inserting the needle approximately 0.5 cm at four sites (i.e., the 3, 6, 9, and 12 o'clock positions), approximately 10 to 15 mL of a 2 percent lidocaine solution is injected. Alternatively, two injection sites at 3 and 9 o'clock positions may be used, or the entire cervix can be anesthetized using multiple injections in a cufflike fashion around the circumference.
Dorsal Penile Block
Dorsal penile block is the most commonly recommended anesthetic technique for neonatal circumcision.11 The needle is inserted at the 2 o'clock position at the base of the penis with slight medial angulation and is advanced approximately 0.5 cm beneath the skin surface, and 0.5 mL of a 1 percent lidocaine solution without epinephrine is injected. The needle is withdrawn, and the injection is repeated at the 10 o'clock position. Applying a topical anesthetic cream (e.g., eutectic mixture of local anesthetics [EMLA] cream) over the skin to be circumcised is a safe and effective alternative.12
