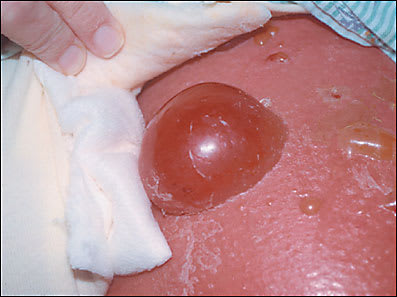
A 50-year-old man in the intensive care unit has large bullae bilaterally on his inner thighs (see accompanying figure). The patient was admitted two days before the onset of the blisters with congestive heart failure and renal failure. On the day before the dermatology consult, the patient was started on intravenous vancomycin for presumed bilateral lower extremity cellulitis. The blisters were tense, filled with clear fluid, and measured about 1 to 3 cm in size.
Question
Based on the patient’s history and physical examination, which one of the following is the correct diagnosis?
A. Bullae secondary to edema.
B. Bullous pemphigoid.
C. Pemphigus vulgaris.
D. Herpes zoster.
E. Fixed drug reaction.
Discussion
Answer is A: Bullae secondary to edema. Patients with fluid overload may present with blister formation, especially on the extremities such as occurred with this patient. When the cause of the underlying edema is treated, the blisters subside. Blisters that form because of edema contain sterile fluid. Because of their thin roof, they usually break within a few days. Once the fluid imbalance is corrected, these blisters resolve without recurrence.1 If the blisters are located on a distal portion of the lower extremities, elevation of the legs can reduce the edema and subsequent blister formation.
Bullous pemphigoid is an autoimmune disease that typically occurs in older patients. Men are affected more commonly than women. Blisters appear on the extremities and intertriginous areas first and later involve the trunk. Intact blisters tend to outnumber erosions in pemphigoid, while the reverse is true of the more superficial blisters occurring in pemphigus.
Pemphigus vulgaris is another autoimmune blistering disease. Patients present with painful bullae that appear on normal skin without surrounding inflammation.2 Lesions often start in the oral mucosa and may precede other cutaneous lesions by several weeks or months. The blister can be extended easily into adjacent skin with gentle pressure (Nikolsky’s sign). Because pemphigus vesicles are thin-roofed, erosions typically outnumber intact blisters. After a blister breaks, the shallow erosion in the skin may take weeks or months to heal.
Varicella zoster virus is a herpes family virus commonly known as chickenpox. The recurrence of varicella zoster is known as herpes zoster, which is recognized by the unilateral dermatomal distribution of vesicles. The large size and bilateral distribution of the blisters in this case would make zoster unlikely.
A fixed drug reaction typically presents with bulla formation on an erythematous base. This fixed reaction reappears in the same site each time the causative drug is ingested.3 Salicylates, nonsteroidal anti-inflammatory drugs, barbiturates, tetracycline, and sulfonamides are among the drugs most commonly cited as causes of fixed drug reactions. The most common cutaneous reaction associated with vancomycin is an urticarial rash, but it also may cause red-man syndrome, toxic epidermolysis necrolysis, or Stevens-Johnson syndrome.
Selected Differential Diagnosis of Blisters
| Condition | Characteristics |
|---|---|
| Bullae secondary to edema | Bullae on lower extremities with associated edema |
| Bullous pemphigoid | Tense vesicles and bullae |
| Pemphigus vulgaris | Flaccid, easily ruptured vesicles |
| Herpes zoster | Follows dermatome, small vesicles |
| Fixed drug reaction | Localized lesion or cluster reappears at same site on rechallenge |
