
Am Fam Physician. 2005;71(12):2353-2355
A 37-year-old Greek woman presented to her physician’s office for a routine physical examination. She did not complain of any symptoms or active medical problems. Her medical history was notable only for mitral valve prolapse. She did not smoke, drink alcohol, or use illicit drugs. Physical examination revealed a II/VI systolic murmur over the mitral area. Deep palpation of the right upper abdominal quadrant caused mild discomfort and pain. Results of the rest of the physical examination were normal.
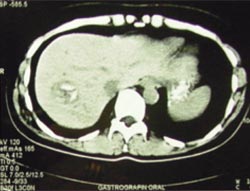
The patient underwent laboratory and imaging testing to evaluate tenderness of the right upper abdominal quadrant that was noted during physical examination. The laboratory testing, which included complete blood count and measurement of serum glucose, creatinine, total lipid, cholesterol, triglyceride, alanine transaminase, aspartate transaminase, gamma glutamyl transpeptidase, and alkaline phosphatase levels, did not reveal any abnormal findings. The erythrocyte sedimentation rate was elevated slightly (26 mm in the first hour [normal values less than 20 mm]). Ultrasonography of the right upper quadrant revealed a well-circumscribed mass with mixed echographic pattern in the right hepatic lobe. Contrast-enhanced computed tomography (CT) of the abdomen was performed subsequently (Figures 1 and 2).

Question
Discussion
The answer is D: echinococcal cyst. Solitary or multiple cystic lesions of the liver may be caused by a variety of conditions, including primary and metastatic neoplasms, non-neoplastic cysts, and infections.1 Echinococciasis (hydatid cyst) is a parasitic disease most often caused by Echinococcus granulosus. Dogs are the host animal, passing eggs in their feces. Echinococciasis always should be included in the differential diagnosis of symptomatic or asymptomatic right upper quadrant masses, particularly in patients who are from or have traveled to endemic areas. Extrahepatic sites include the bones, brain, and lungs.
Ultrasonography and CT imaging are the cornerstone for the diagnosis, classification of the stage of progression, and determination of the best mode of treatment. Blood tests are available, although the limitations of serum testing should be taken into consideration: the sensitivity of serum echinococcal antigens ranges from 80 to 95 percent for hepatic-limited echinococcal disease, and is lower for solitary extrahepatic echinococcal cysts.2,3 Specificity ranges from 88 to 96 percent.3 Needle biopsy and cyst aspiration are options, but often are avoided because of the risk of cyst rupture.
The CT imaging in this patient is not typical of echinococciasis. Echinococcal cyst can lead to peculiar findings on different imaging techniques, depending on which parts of the cyst are captured in the image and on the stage of disease. Although CT sections of the lower and central part of the lesion exhibited the typical well-demarcated, hypodense cyst (Figure 1),4 CT sections of the upper part of the lesion exhibited hyperdense, separated, peripheral areas (Figure 2). They may represent calcified daughter hydatid cysts5 separated by fibrous tissue or, more likely, a redundant, folded, inner germinal wall of a cyst.1
Serum echinococcal antigens were negative in this patient, but biopsy of the excised specimen confirmed the diagnosis of echinococciasis. Treatment included surgical excision of the mass, with 400 mg of albendazole per day for one week before and two weeks after surgery.
Hepatocellular carcinoma is unlikely because of the imaging characteristics of the liver lesion. Usually, such lesions would have irregular borders. In most patients, hepatocellular carcinoma presents after the fifth decade of life, and is related to a history of chronic liver disease (e.g., viral hepatitis, cirrhosis).
Pyogenic liver abscess usually manifests with fever. Chills, rigors, or malaise also may be present, and some patients appear to be septic.
A simple cyst of the liver does not have calcified areas. In addition, simple cysts do not have mixed echogenic characteristics unless they are infected or hemorrhagic.
Liver metastases frequently present with multiple hepatic lesions on diagnosis. Usually the patient already has symptoms and or signs from the primary cancer.
| Condition | Characteristics |
|---|---|
| Hepatocellular carcinoma | Commonly related to previous chronic hepatic disease |
| Pyogenic liver abscess | Usually manifests with fever, chills, rigors, or malaise |
| Simple liver cyst | Silent clinical course; symptomatic only if cyst becomes infected or ruptures |
| Echinococciasis hydatid cyst(Echinococcus granulosus) | Endemic in many areas of the world; chronic clinical course; dramatic anaphylactic reaction if cyst ruptures; characteristic cystic appearance on imaging |
| Metastatic cancer of the liver | Frequently presents with multiple hepatic lesions; usually symptoms and/or signs from the primary site of cancer |