
Am Fam Physician. 2007;75(5):707-708
Author disclosure: Nothing to disclose.
An 84-year-old man had chest radiography six months after coronary artery bypass grafting and was found to have a solitary pulmonary nodule. It was located in the right lung and measured approximately 1.5 cm in diameter. He had no other complaints. Because of his age and recent surgery, invasive diagnostic procedures were initially deferred.
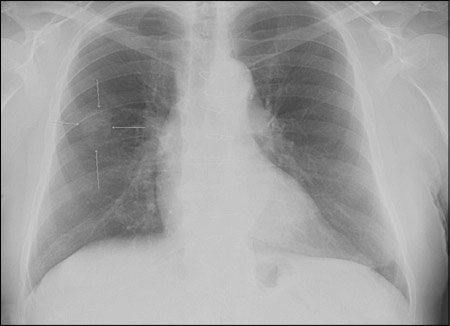
Follow-up chest radiography (Figure 1) showed the nodule had grown to 2.5 cm in diameter. The patient was still in good physical condition and was asymptomatic except for the recent onset of mild fatigue and mild exertional dyspnea. Laboratory testing revealed no abnormalities.
Question
Discussion
The answer is A: carcinoma. A solitary pulmonary nodule is an isolated, radiologically visible mass less than 3 cm in diameter without associated atelectasis or adenopathy.1–3 These nodules are relatively common; they are found in one in 500 patients during routine chest radiography.2,4 They may represent a variety of lesions that are neoplastic, hamartomatous, infectious, vascular, or artifact. Although many such lesions are malignant, some are benign. Pathologic lesions accounting for 5 percent or more of all solitary pulmonary nodules are listed in the accompanying table.1
When chest radiography reveals a solitary nodule, comparison with previous chest films is important because nodules that are unchanged after two years do not require further work-up.2,3 For new or enlarging nodules 1 cm or more in diameter, high-resolution computed tomography (CT) is the next diagnostic step.3 If the nodule is suspicious on CT scan, positron emission tomography (PET) with radioactive glucose (fludeoxyglucose F 18) can be performed. This is a noninvasive way to evaluate whether the lesion is metabolically quiescent (benign) or metabolically active (suggesting malignancy, infection, or inflammation). If it is metabolically active, the PET scan can be used to evaluate for corresponding adenopathy or metastasis. Fine-needle aspiration for peripheral lesions and bronchoscopy for central lesions can yield a tissue diagnosis but are operator dependent and somewhat invasive.3,4 If the biopsy tissue is positive for non–small cell lung cancer, adequate staging via PET scan will determine whether the patient is a candidate for surgery, chemotherapy, or radiation therapy.5
For solitary pulmonary nodules 1 cm or less in diameter, the algorithm is different in patients with low clinical suspicion for cancer versus patients with intermediate to high clinical suspicion.5 Watchful waiting with CT follow-up is preferred for patients with low clinical suspicion; high-resolution CT is recommended for those with moderate to high clinical suspicion.3
Fungal granulomas, especially those caused by Histoplasma capsulatum, may resemble tuberculomas. They are round or oval, sharply circumscribed nodules; are usually less than 3 cm in diameter; and are often associated with calcified hilar lymph nodes. Central calcifications are common.6
Pulmonary hamartoma is an unlikely finding in older men. On radiographic examination, pulmonary hamartomas appear lobulated; well circumscribed; and, in 10 to 20 percent of cases, contain “popcorn” calcification (i.e., multiple punctuate calcifications in the lesion).6 The finding of fat within the lesion is pathognomonic, but usually this can only be confirmed by CT scan. Hamartomas do not tend to grow and often can be found on previous radiographic films.
Radiographic artifacts (e.g., nipples, skin nodules, vertebral osteophytes) may be mistaken for solitary pulmonary nodules. Physical examination of the film and the patient is essential. A repeat film with nipple or skin markers, or oblique or lordotic views often clarify skin and bone lesions. Pleural plaques are harder to discern. The lesion should be visible on both the posterior-anterior and lateral views to confirm it is truly a nodule (i.e., has three dimensions). If there is sufficient clinical concern or doubt, CT is indicated.
Tuberculoma usually presents as an upper lobe nodule with central calcification. It often is associated with “satellite” lesions. These may be bilateral, and typically are accompanied by enlargement and calcification of the hilar lymph nodes.6
| Condition | Characteristics |
|---|---|
| Carcinoma | Primary: usually spiculated, not calcified; metastatic: usually round, multiple, not calcified |
| Fungal granuloma | Round or oval, often multiple nodules; usually calcified; often with calcified hilar nodes |
| Hamartoma | Lobulated, well circumscribed; 10 to 20 percent have “popcorn” calcification; finding of fat within is pathognomonic |
| Radiographic artifacts | Physical examination and repeat film to clarify bone and skin lesions; lesion visible on both posterior-anterior and lateral views |
| Tuberculoma | Central calcification and “satellite” lesions, usually with calcification of hilar lymph nodes |