
Am Fam Physician. 2007;76(12):1853-1854
Author disclosure: Nothing to disclose.
A 73-year-old man with a history of type 2 diabetes presented with right upper quadrant abdominal pain and fever. Physical examination revealed that the patient had tenderness in the right upper quadrant and a temperature of 100.4° F (38° C). Laboratory studies showed a white blood cell count of 15,500 cells per mm3 (15.5 × 109 per L), with 87 percent neutrophils; an alkaline phosphatase level of 158 U per L (2.64 μkat per L); and a total serum bilirubin level of 1.7 mg per dL (29 μmol per L). Plain abdominal radiography was performed (Figure 1).

Question
Discussion
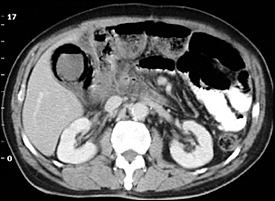
The answer is A: emphysematous chole-cystitis. Emphysematous cholecystitis is characterized by gas accumulation in the gallbladder lumen, wall, or pericholecystic tissue, which can be seen in imaging studies. This patient's plain abdominal radiograph shows oval-shaped gas accumulation in the gallbladder lumen and linear gas outlining the wall (Figure 1); computed tomography (CT) confirms these findings (Figure 2).
Emphysematous cholecystitis is a rare but serious manifestation of acute cholecystitis. It is most common in older men with diabetes and has a 15 percent mortality rate.1 It is caused by proliferation of gas-forming organisms (e.g., Clostridium perfringens, Escherichia coli) after vascular compromise of the gallbladder.
Initially, symptoms of emphysematous cholecystitis are indistinguishable from those of uncomplicated acute cholecystitis: right upper quadrant pain radiating to the back, vomiting, fever, and chills. However, because older patients with diabetes may have few or no localizing symptoms or signs, emphysematous cholecystitis should be considered early in at-risk patients.2,3 Emphysematous cholecystitis requires immediate cholecystectomy and broad-spectrum antibiotic therapy.1,2
A diagnosis of emphysematous cholecystitis can be confirmed with plain radiography, ultrasonography, or CT. Plain radiography may be sufficient but has low sensitivity early in the disease.4 Ultrasound findings suggestive of the condition depend on the amount and location of the gas.5 CT is the most definitive modality when findings on plain radiography or ultrasonography are equivocal.4
Emphysematous pyelonephritis is a severe, necrotizing infection of the renal parenchyma caused by gas formation in the collecting system, renal parenchyma, or perirenal tissues. Signs and symptoms are similar to those of acute pyelonephritis. There may be streaky, mottled gas distribution over the infected renal fossa that is associated with an ileus pattern.
Liver abscesses may be associated with amorphous gas collection in the liver (as many as 20 percent of cases) or basilar atelectasis, right hemidiaphragm elevation, and right pleural effusion (about 50 percent of cases).
Pneumobilia is usually secondary to biliary-enteric fistula (spontaneous or surgical), incompetent sphincter of Oddi, biliary-enteric anastomosis (surgical), or cholangitis caused by gas-forming organisms. Spherical, linear, branching gas accumulation in the liver shown on a plain abdominal radiograph represents gas within the intrahepatic biliary duct system.
Pneumoperitoneum often is caused by perforation of the hollow organs. Supine plain abdominal radiographs may show triangular gas accumulation in Morison's pouch, oblong gas accumulation in the subhepatic space, circular gas accumulation over the liver (between the anterior liver surface and abdominal wall), and parahepatic gas bubbles lateral to the right edge of the liver.
| Condition | Characteristics |
|---|---|
| Emphysematous cholecystitis | Gas accumulation in the gallbladder lumen or pericholecystic tissue and linear gas within the wall |
| Emphysematous pyelonephritis | Streaky, mottled gas distribution over the infected renal fossa that is associated with an ileus pattern |
| Liver abscess | Amorphous gas accumulation in the liver is possible; basilar atelectasis, right hemidiaphragm elevation, and right pleural effusion |
| Pneumobilia | Spherical, linear, branching gas accumulation in the liver |
| Pneumoperitoneum | Triangular gas accumulation in Morison's pouch, oblong accumulation in the subhepatic space, circular accumulation over the liver, and parahepatic gas bubbles lateral to the right edge of the liver |