Skin laceration repair is an important skill in family medicine. Sutures, tissue adhesives, staples, and skin-closure tapes are options in the outpatient setting. Physicians should be familiar with various suturing techniques, including simple, running, and half-buried mattress (corner) sutures. Although suturing is the preferred method for laceration repair, tissue adhesives are similar in patient satisfaction, infection rates, and scarring risk in low skin-tension areas and may be more cost-effective. The tissue adhesive hair apposition technique also is effective in repairing scalp lacerations. The sting of local anesthesia injections can be lessened by using smaller gauge needles, administering the injection slowly, and warming or buffering the solution. Studies have shown that tap water is safe to use for irrigation, that white petrolatum ointment is as effective as antibiotic ointment in postprocedure care, and that wetting the wound as early as 12 hours after repair does not increase the risk of infection. Patient education and appropriate procedural coding are important after the repair.
Although the emergency department routinely treats acute trauma, family physicians should be prepared to manage acute lacerations. This requires knowledge of wound evaluation, preparation, and appropriate repair techniques; when to refer for surgical treatment; and how to provide follow-up care.
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | References |
|---|---|---|
| Saline or tap water may be used for wound irrigation, whereas povidone-iodine, detergents, and hydrogen peroxide should be avoided. | B | 3, 5 |
| The sting from a local anesthetic injection can be decreased by slow administration and buffering the solution. | B | 8 |
| Suturing is the preferred technique for skin laceration repair. | C | 5 |
| Tissue adhesives are comparable with sutures in cosmetic results, dehiscence rates, and infection risk. | A | 14–17 |
| Applying white petrolatum to a sterile wound to promote wound healing is as effective as applying an antibiotic ointment. | B | 25 |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.xml.
Wound Evaluation and Preparation
Immediately upon presentation, a laceration should be evaluated and the bleeding controlled using direct pressure. A patient history should be obtained, including mechanism and time of injury and personal health information (e.g., human immunodeficiency virus and diabetes status; tetanus immunization history; allergies to latex, local anesthesia, tape, or antibiotics). A careful exploration of the laceration should be performed to determine severity and whether it involves muscle, tendons, nerves, blood vessels, or bone. Baseline neurovascular and functional status of the involved body part should be evaluated before repair. Lacerations that expose underlying tissue or continue bleeding should be repaired, although some less severe wounds (e.g., simple hand lacerations that are less than 2 cm long) may heal well with conservative management.1
The goals of laceration repair are to achieve hemostasis, avoid infection, restore function to the involved tissues, and achieve optimal cosmetic results with minimal scarring. Definitive laceration management depends on the time since injury, the extent and location of the wound, available laceration repair materials, and the skill of the physician. Guidelines for seeking surgical consultation for laceration repair are presented in Table 1.
Table 1 Guidelines for Seeking Surgical Consultation for Laceration Repair
| Deep wounds of the hand or foot |
| Full-thickness lacerations of the eyelid, lip, or ear |
| Lacerations involving nerves, arteries, bones, or joints |
| Penetrating wounds of unknown depth |
| Severe crush injuries |
| Severely contaminated wounds requiring drainage |
| Wounds leading to a strong concern about cosmetic outcome |
note: Surgical consultation should be considered for these wounds; however, referral decisions are ultimately based on the physician's level of expertise, experience, and comfort with managing the laceration.
The optimal time interval from injury to laceration repair is not clearly defined. Anatomic location of the wound, health of the patient, mechanism of injury, and wound contamination factor into the decision about when to repair the laceration. Noncontaminated wounds have been successfully closed up to 12 hours post-injury.2 Clean lacerations involving well-vascularized tissue, such as the face and scalp, can be closed successfully even later in healthy patients, although risk of infection must be minimized. Regardless of location, these older lacerations can be repaired with loose, single interrupted sutures that are sufficient to close the wound. Alternatively, if no wound infection develops, the wound may be packed for three to five days followed by delayed primary closure. If infection occurs, the wound should be allowed to heal by secondary intention. Both methods take into account potential wound infection and offer the potential for an acceptable cosmetic result.
Copious wound irrigation with normal saline or tap water 3 washes away foreign matter and dilutes the bacterial concentration to decrease post-repair infection. Warmed irrigation solution is more comfortable for the patient.4 Povidone-iodine solution, hydrogen peroxide, and detergents should not be used because their toxicity to fibro-blasts impedes healing.5 The wound should be irrigated copiously with a 30- to 60-mL syringe and 18-gauge needle or angiocatheter, which can cleanse at 5 to 8 lb per square inch of pressure without damaging the tissue.6 Any visible foreign matter should be removed with forceps, and devitalized tissue removed with sharp debridement to reduce the risk of infection. Foreign bodies near blood vessels, nerves, and joints should be removed with caution, and surgical referral should be considered. Local hair should be clipped, not shaved, to prevent wound contamination7; clipping of the eyebrows should be avoided because of unpredictable regrowth and to prevent uneven reapproximation.
Local anesthesia with lidocaine 1% (Xylocaine; 10 mg per mL) or bupivacaine 0.25% (Marcaine; 2.5 mg per mL) is appropriate for small wounds, if needed. Large wounds occurring on limbs may require a regional block to prevent toxic doses of the local anesthetic (lidocaine 3 to 5 mg per kg without epinephrine, and up to 7 mg per kg with epinephrine; bupivacaine 1 to 2 mg per kg without epinephrine, and up to 3 mg per kg with epinephrine). Epinephrine, which is used to decrease wound bleeding through vasoconstriction, should be avoided when wounds involve anatomic areas with end arterioles, such as the digits, nose, penis, and earlobes. The sting of local anesthetic injections may be reduced by using a smaller needle (25 to 30 gauge), injecting slowly,8 warming the anesthetic solution, or buffering the solution with sodium bicarbonate 8.4% (1 mL of sodium bicarbonate per 10 mL of local anesthetic). In persons who are allergic to amide forms of local anesthetics, intradermal diphenhydramine 1% (created by adding 1 mL of diphenhydramine, 50 mg per mL solution, to 4 mL of sterile saline) may be substituted because it has local anesthetic effects. Topical anesthetics, such as lidocaine/prilocaine cream (EMLA), also may be used, especially in children and in patients who cannot tolerate injections. The cream is applied to intact skin and covered with an occlusive dressing one to four hours before the repair procedure. In newborns, a maximum application of one hour is suggested to avoid the theoretic risk of acquired methemoglobinemia.9
Laceration Repair Techniques
Laceration repair options in the outpatient setting include sutures, tissue adhesives, staples, and skin-closure tape. Physicians should have a working knowledge of these techniques, including how to choose the correct closure method and how to perform closures to obtain optimal results. Wounds requiring extensive debridement or multiple-layer closure are best repaired with a suture. Areas of high skin tension, such as over joints, or areas with a thick dermis, such as on the back, should be repaired with sutures or staples. Areas with low skin tension, such as on the face, shin, and dorsal hand, may be effectively repaired with tissue adhesives, especially in children.10
Laceration repair techniques follow common principles, regardless of laceration location or closure method. Aseptic techniques must be used, including sterile fields and gloves and universal body fluid precautions. Deep wounds require a multiple-layer closure with an absorbable suture and possibly a temporary drain to reduce the risk of hematoma or subsequent infections. A multiple-layer closure can improve cosmetic results by bringing opposing wound edges closer together and decreasing wound tension.
SUTURING
Suturing is the preferred technique for laceration repair.5 Absorbable sutures, such as polyglactin 910 (Vicryl), polyglycolic acid (Dexon), and poliglecaprone 25 (Monocryl), are used to close deep, multiple-layer lacerations. Although these sutures absorb at varying rates, they all usually absorb within four to eight weeks. Nylon, monofilament nonabsorbable sutures (e.g., polypropylene [Prolene]) must eventually be removed. The role of absorbable sutures in the closure of areas with low skin tension continues to be evaluated. The wound dehiscence rate, cosmetic results, and infection risk of absorbable sutures appear to be comparable to that of nonabsorbable sutures, and absorbable sutures are more cost-effective because there is no need for removal.11,12 Silk sutures are no longer used to close the skin because of their poor tensile strength and high tissue reactivity.
Optimal cosmetic results can be achieved by using the finest suture possible, depending on skin thickness and wound tension. In general, a 3–0 or 4–0 suture is appropriate on the trunk, 4–0 or 5–0 on the extremities and scalp, and 5–0 or 6–0 on the face. Blue-colored sutures may be beneficial for scalp lacerations in appropriate populations to differentiate the suture from the hair.
Mucosal lacerations (e.g., mouth, tongue, genitalia) with significant hemorrhage or depth that involve muscular layers, or that may have significant functional or cosmetic outcomes, such as a split tongue, should be repaired. An absorbable 3–0 or 4–0 suture should be used.
After the wound is prepped, the appropriate suturing technique must be selected. Deep, multiple-layer wounds should be repaired using absorbable, single interrupted sutures (Figure 1A). Most other wounds can be closed effectively with nonabsorbable, single interrupted sutures. The needle should pierce the skin at a 90-degree angle with the trailing suture following the curve of the needle, which is accomplished by twisting the wrist. This technique will cause eversion of the wound edges (Figure 2), compensating for the eventual retraction of the scar during healing.13 Traditionally, the suture begins in the middle of the wound, with the remaining stitches placed symmetrically until the wound is closed.
Figure 1.
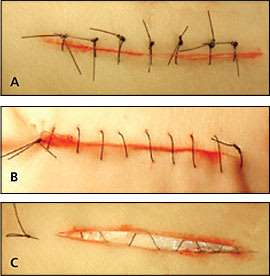
Suture techniques for laceration repair. (A) Single interrupted closure. (B) Running (“baseball”) closure. (C) Subcuticular running closure.
Figure 2.
Proper technique of a single interrupted stitch for wound eversion and closure. The needle should pierce the skin at a 90-degree angle with the trailing suture following the curve of the needle, which is accomplished by twisting the wrist.
The horizontal mattress technique (Figure 3) may be the best option for closing gaping or high-tension wounds or wounds on fragile skin because it spreads the tension along the wound edge. The vertical mattress technique (Figure 4) is best for everting wound edges in areas that tend to invert, such as the posterior neck or concave skin surfaces.14 A variation, called the half-buried mattress (corner) suture (Figure 5), is ideal for closure of a triangular edge because it does not compromise the blood supply, theoretically decreasing tip necrosis. A running (“baseball”) suture (Figure 1B) is used for long, low-tension wounds, whereas a subcuticular running suture (Figure 1C) is ideal for closing small lacerations in low skin-tension areas where cosmesis is important, such as on the face. The ends of this suture do not need to be tied, but they may be secured with slip knots or tape.
Figure 3.
Horizontal mattress suture technique.
Figure 4.
Vertical mattress suture technique.
Figure 5.
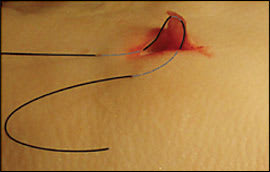
Half-buried mattress (corner) suture for laceration repair. Note that the suture remains subcuticular in the flap to avoid cutting off the blood supply.
After the repair is complete, the wound should be cleaned with sterile saline and dressed appropriately. Lacerations over joints may be splinted temporarily for comfort and to promote healing.
TISSUE ADHESIVES
Tissue adhesives, such as 2-octylcyanoacrylate (Dermabond), are comparable with sutures in cosmetic results, dehiscence rates, and infection risk.15–17 However, tissue adhesives can be applied more quickly, require no anesthesia, and eliminate the need for follow-up because they slough off spontaneously within five to 10 days. They form a protective barrier to promote wound healing and may have antimicrobial effects.18 Although tissue adhesives have a higher direct cost per unit than sutures, they are more cost-effective because of quick application and no follow-up.19 Tissue adhesives' low tensile strength makes them inappropriate for high-tension areas, such as over joints, unless the area is immobilized. They may be ideal for simple lacerations under a cast or splint. Tissue adhesives are contraindicated in patients at higher risk of poor healing (e.g., those who are immunosuppressed or have diabetes), and should not be used for contaminated, complex, or jagged lacerations. They should also be avoided on mucosal surfaces and areas that maintain moisture, such as the groin or axillae.15
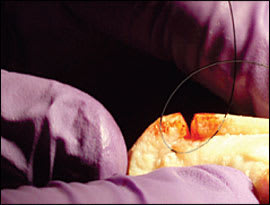
Effective application of tissue adhesives is a quickly learned skill compared with suturing.20 Figure 6 shows the proper technique. After irrigation, the wound should be dried with sterile gauze and placed in a horizontal position to prevent runoff, using caution around the eyes. The wound edges are approximated using gloved fingers, then the adhesive is applied in a thin layer over the wound with a 5-mm overlap on each side. Three to four layers are applied with 30 seconds between applications. Full tensile strength is achieved after 2.5 minutes. Antibiotic and white petrolatum ointments can remove tissue adhesive; therefore, patients must be instructed to avoid using them on the repaired wound.
Figure 6.

Proper technique for the application of tissue adhesive in laceration repair. Note the wound edge approximation and thin layer of tissue adhesive.
The hair apposition technique (Figure 7) may be used for closing scalp wounds. The technique is best for non-actively bleeding wounds that are less than 10 cm long when scalp hair is longer than 3 cm. Opposing strands of hair are brought together with a simple twist and are secured with a drop of tissue adhesive. The technique can be performed by nonphysicians and causes less scarring, has fewer complications,21 and is more cost-effective than a scalp suture.22
Figure 7.
Hair apposition suture technique.
OTHER TECHNIQUES
Stainless steel or absorbable staples and skin-closure strips (e.g., Steri-strips) are also commonly used to repair lacerations. Automatic staplers, usually used in surgical wound repair, are recommended for closing thick skin on the extremities, trunk, and scalp, but not on the face, neck, hands, and feet. Stainless steel staples should not be used for scalp wounds if computed tomography or magnetic resonance imaging of the head is anticipated. The quick application of staples makes them a good choice for patients who have multiple traumas or who are intoxicated.
Although skin-closure strips can be effective for small, simple lacerations in low-tension areas with well-approximated edges, their lack of tensile strength can lead to wound dehiscence. Also, adhesive adjuncts, such as tincture of benzoin, can cause a local inflammatory reaction. However, skin-closure strips have a role in the repair of pretibial lacerations, leading to faster wound healing and less necrosis.23
Follow-up Care and Billing
Follow-up for repaired lacerations is similar regardless of the technique used. Traditionally, patients have been told to keep the wound clean and dry using a protective dressing for at least 24 hours after the repair procedure. However, one study showed that leaving the wound uncovered and wetting it after 12 hours did not increase infection rates.24 To prevent infection and promote healing, an antibiotic or white petrolatum ointment can be applied daily to wounds not repaired with tissue adhesives. Antibiotic and white petrolatum ointments are equally effective.25,26 The timing of suture or staple removal varies with wound location (Table 2).
Table 2 Timing of Suture or Staple Removal
| Wound location | Timing of removal (days) |
|---|---|
| Face | Three to five |
| Scalp | Seven to 10 |
| Arms | Seven to 10 |
| Trunk | 10 to 14 |
| Legs | 10 to 14 |
| Hands or feet | 10 to 14 |
| Palms or soles | 14 to 21 |
Tetanus immunization status should be assessed in patients with lacerations. Table 3 summarizes the Centers for Disease Control and Prevention guidelines for tetanus pro-phylaxis in these patients.27 After laceration repair, patients should receive instructions on signs of infection and when follow-up should be performed (see accompanying patient education handout).
Table 3 Guidelines for Tetanus Prophylaxis in Adults Receiving Routine Wound Management
| History of absorbed tetanus toxoid | Clean, minor wound | All other wounds* | ||
|---|---|---|---|---|
| Tdap or Td | TIG | Tdap or Td | TIG | |
| Unknown or less than three doses | Yes | No | Yes | Yes |
| More than three doses | No† | No | No‡ | No |
note: Guidelines apply to adults 19 to 64 years of age.
Td = tetanus-diphtheria toxoids vaccine; Tdap = diphtheria, reduced tetanus toxoids, and acellular pertussis vaccine; TIG = tetanus immune globulin.
*— Such as, but not limited to, wounds contaminated with dirt, feces, soil, or saliva; puncture wound; avulsions; and wounds resulting from missiles, crushing, burns or frostbite.
†— Yes, if it has been 10 years or more since the last dose of tetanus toxoid–containing vaccine.
‡—Yes, if it has been five years or more since the last dose of tetanus toxoid–containing vaccine.
Adapted from Kretsinger K, Broder KR, Cortese MM, et al. Preventing tetanus, diphtheria, and pertussis among adults: use of tetanus toxoid, reduced diphtheria toxoid and acellular pertussis vaccine recommendations of the Advisory Committee on Immunization Practices (ACIP) and recommendation of ACIP, supported by the Healthcare Infection Control Practices Advisory Committee (HICPAC), for use of Tdap among health-care personnel. MMWR Recomm Rep. 2006;55(RR-17):25.
Billing for laceration repair depends on the size and location of the wound and on the complexity of the repair. Table 4 includes codes for common procedures.28 Sutures, staples, and tissue adhesives are all billable methods. Adhesive strips alone should be categorized using the appropriate evaluation and management code. Simple laceration repair includes superficial, single-layer closures with local anesthesia; intermediate laceration repair includes multiple-layer closures or extensive cleaning; and complex laceration repair includes multiple-layer closures, debridement, and other wound preparation (e.g., undermining of skin for better wound edge closure). Follow-up suture removal is included in the laceration repair fee, but can be billed if the repair was performed elsewhere, such as in the emergency department.
Table 4 CPT Codes for Laceration Repairs
| Location of wound | Length of wound (cm) | CPT Code |
|---|---|---|
| Simple repairs | ||
| Scalp, trunk, limbs | 2.5 or less | 12001 |
| 2.6 to 7.5 | 12002 | |
| Face, ears, eyelids | 2.5 or less | 12011 |
| 2.6 to 5.0 | 12013 | |
| 5.1 to 7.5 | 12014 | |
| Intermediate repairs | ||
| Scalp, trunk, limbs | 2.5 or less | 12031 |
| 2.6 to 7.5 | 12032 | |
| 7.6 to 12.5 | 12034 | |
| Neck, hands, feet | 2.5 or less | 12041 |
| 2.6 to 7.5 | 12042 | |
| 7.6 to 12.5 | 12044 | |
| Face, ears, eyelids | 2.5 or less | 12051 |
| 2.6 to 5.0 | 12052 | |
| 5.1 to 7.5 | 12053 | |
CPT = common procedural terminology.
Information from reference 28.
