
Am Fam Physician. 2011;83(8):969-970
Author disclosure: Nothing to disclose.
A 62-year-old man presented with a two-month history of asymptomatic, progressive thickening of both nipples and areolae. Lesions initially appeared on the left side, and then spread to the right side. The involvement of the areolae was more prominent than that of the nipples. The patient had a history of gynecomastia, hypoparathyroidism, and hypogonadism, for which he was using topical testosterone gel and oral ergocalciferol. For more than 10 years, he had regularly administered intramuscular growth hormone for antiaging purposes. He had no personal or family history of cancer. A review of systems was negative for any preceding illness, recent weight loss, or constitutional symptoms.

Question
Discussion
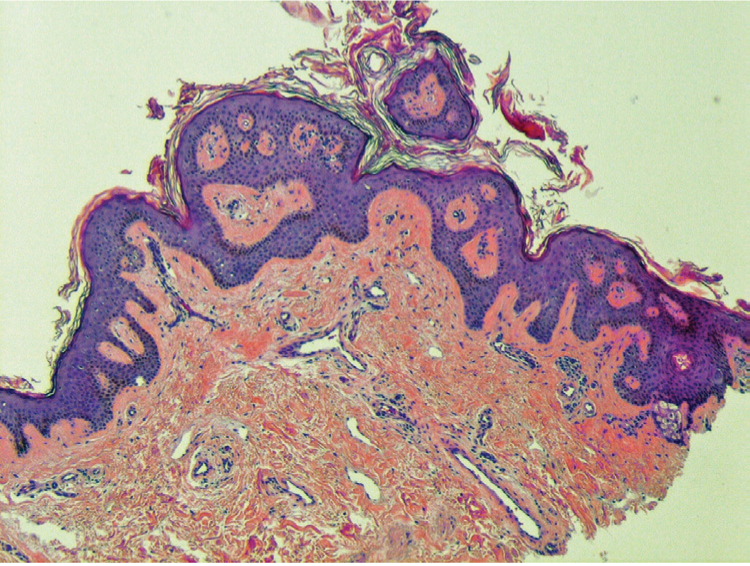
Nevoid hyperkeratosis is characterized by unilateral or bilateral, diffuse, verrucous thickening and brown pigmentation of the nipple, areola, or both. There is typically no erythema, induration, or discharge from the involved area, and patients are usually asymptomatic 2; therefore, the condition is likely underreported. Because nevoid hyperkeratosis may be difficult to distinguish from malignant forms of disease, biopsy is necessary.3 The two most common histologic changes associated with nevoid hyperkeratosis are extreme hyperkeratosis and papillomatosis, but acanthosis and keratotic plugging are also reported.3,4
There are no specific treatment guidelines for nevoid hyperkeratosis. However, several therapeutic measures have been used for cosmesis with variable success, including topical corticosteroids, keratolytics, tretinoin (Retin-A), calcipotriene (Dovonex), etretinate (not available in the United States), radiofrequency therapy, surgery, cryosurgery, and shave excision.4
Darier disease is a disorder of keratinization that usually occurs through autosomal dominant inheritance.5 It can cause hyperkeratosis of the nipples, but other areas are also usually affected. The disease typically appears as an acneiform eruption on the chest, back, scalp, neck, and forehead. Histologically, Darier disease is defined by dyskeratosis and acantholysis, which distinguish it from nevoid hyperkeratosis.
Paget disease of the breast is a disorder of the nipple-areola complex that commonly leads to pruritus and burning.6 It is often associated with underlying in situ or invasive carcinoma. Eczematous changes of the skin may include erythema, scaling, and lichenification, which may progress to ulceration or total destruction of the region. In this case, histology would show a neoplastic process with disarray of the cellular architecture.2
Seborrheic keratosis typically appears as sharply demarcated plaques or papules, contrary to the diffuse plaques in nevoid hyperkeratosis of the nipple and areola.1 The two conditions can also be distinguished histopathologically, with seborrheic keratosis largely showing basaloid cell acanthosis and no papillomatosis.
| Condition | Characteristics |
|---|---|
| Darier disease | Acneiform lesions on the chest, back, scalp, neck, and forehead; hyperkeratosis of the nipples possible; histology shows dyskeratosis and acantholysis |
| Nevoid hyperkeratosis | Unilateral or bilateral, diffuse, verrucous thickening and brown pigmentation of the nipple and/or areola; typically no erythema, induration, or discharge from involved area; histology commonly shows hyperkeratosis and papillomatosis |
| Paget disease of the breast | Disorder of nipple-areola complex that commonly leads to pruritus, burning, and/or eczematous changes; often associated with in situ or invasive carcinoma; histology may show a neoplastic process with disarray of cellular architecture |
| Seborrheic keratosis | Sharply demarcated plaques or papules; histology shows basaloid cell acanthosis and no papillomatosis |
