
Am Fam Physician. 2013;87(2):127-128
Author disclosure: No relevant financial affiliations to disclose.
A 46-year-old man presented to the emergency department with unilateral pain in his left eye that began one day earlier. He had redness and a foreign body sensation. There were no vision changes, discharge, trauma, or recent upper respiratory tract symptoms.
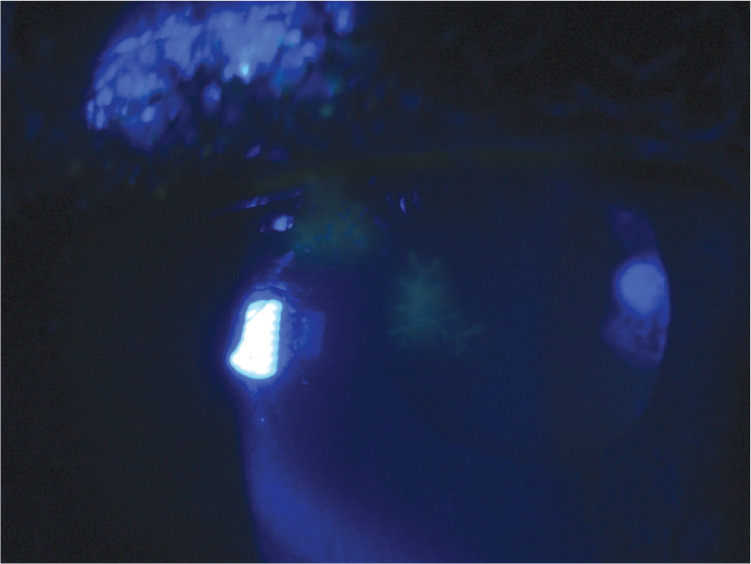
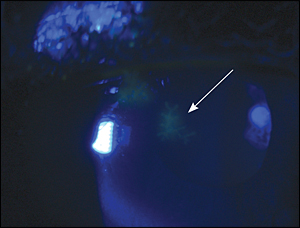
On examination, his pupils were reactive to light with normal ocular motor function. He had consensual photophobia. Slit lamp examination showed ciliary flush and cell flaring, but no conjunctival injection. The patient was further evaluated with fluorescein staining (Figure 1).
Question
Discussion
The answer is C: herpes keratitis. Herpes simplex virus is one of the leading causes of infectious keratitis resulting in blindness. Herpes keratitis is the most common ocular form of herpes infection and usually presents as an infection of the superficial epithelium with dendritic lesions in this layer.1 Symptoms of herpes keratitis vary but may include pain, blurred vision, sensitivity to light, red eye, watery discharge, or foreign body sensation. Recurrent episodes are common.
Patients with a foreign body may have excruciating pain, tearing, and a scratchy sensation with blinking. Slit lamp examination may reveal a foreign body in the anterior or posterior chamber. However, if the object is not present, fluorescein staining may demonstrate a corneal epithelial injury or defect.1
Patients with fungal keratitis may have a history of trauma with vegetative matter, or long-term steroid use.1,3 Common symptoms include pain, red eye, foreign body sensation, and discharge. Typical slit light examination findings include a dry, gray, elevated infiltrate and satellite lesions. Diagnosis requires laboratory confirmation using a fungal culture.
Ocular sarcoidosis can manifest before the presentation of systemic sarcoidosis. Uveitis is a common ocular manifestation of sarcoidosis.4 Examination shows redness in the corneal area. Patients present with bilateral ocular pain, photophobia, and decreased vision, and granuloma formation can be seen in the conjunctiva and uvea.
| Condition | Examination findings | Characteristics |
|---|---|---|
| Foreign body | Foreign body in anterior or posterior chamber; corneal epithelial injury/defect | Excruciating pain, tearing, scratchy sensation with blinking |
| Fungal keratitis | Dry, gray, elevated infiltrate, and satellite lesions | History of trauma with vegetative matter, or long- term steroid use; pain, red eye, foreign body sensation, or discharge |
| Herpes keratitis | Dendritic lesions in the epithelial layer | Pain, blurred vision, sensitivity to light, red eye, foreign body sensation, or watery discharge |
| Uveitis from sarcoidosis | Redness in corneal area, decreased visual acuity | Bilateral ocular pain and photophobia; granuloma formation in the conjunctiva and uvea |
