
Am Fam Physician. 2016;94(10):836-842
Author disclosure: No relevant financial affiliations.
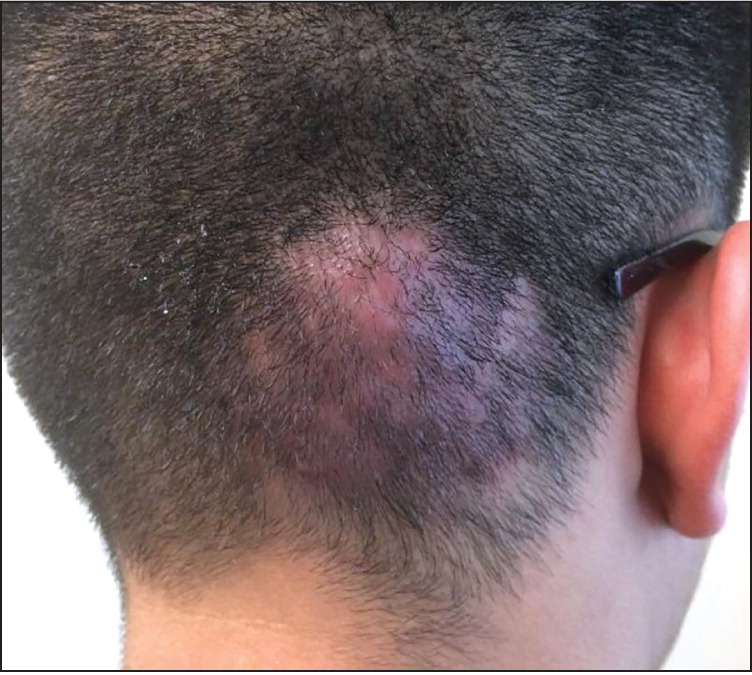
A 16-year-old boy presented with swelling and erythema on the scalp that had worsened over the previous four weeks. Three to four months prior to the development of the swelling, he noted a red circular rash on the same area of his scalp. The rash resolved with application of an over-the-counter antifungal cream. After resolution of the rash, the swelling and erythema began, and the area became painful. He did not have a fever or chills, and there was no discharge from the site. The patient was otherwise healthy and active, and was a member of his school's wrestling team.
Examination of the scalp revealed an area of erythema and induration (Figure 1). The scalp was tender to palpation but not fluctuant. There was no cervical or occipital lymphadenopathy. Ultrasonography showed no fluid collection in the lesion.
Question
Discussion
The answer is B: kerion. Kerions are the result of an inflammatory response to an invasive fungal infection of the hair follicles and scalp. The fungus is usually a dermatophyte such as Trichophyton verrucosum or Trichophyton mentagrophytes.1 Presentation ranges from a raised, spongy lesion to an extremely painful indurated lesion.1 Kerions are commonly mistaken for a staphylococcal abscess, but the absence of fever and fluctuance can help to distinguish them from a bacterial infection. The initial rash is red and circular, which is typical of tinea capitis, a Trichophyton infection that often occurs in wrestlers.
If the fungal infection is untreated, alopecia and scarring may develop. The first-line therapy is oral griseofulvin.2 Topical treatment is not effective because of the depth of the fungal infection. Although bacterial infections can occur with kerions, they are uncommon. Fever, chills, and malaise are common signs of a superimposed bacterial infection, and the lesion is typically fluctuant.3 When there is concern for bacterial superinfection, an antibiotic that covers Staphylococcus and Streptococcus should be used in addition to griseofulvin.
An id reaction, also known as disseminated eczema or autoeczematization, is a generalized acute eczematous reaction that can be triggered by a variety of stimuli, including infection or inflammation. It typically presents as an intensely pruritic, symmetric, maculopapular or papulovesicular rash. Widespread follicular pustules are possible. A focal circular lesion without scaling or lichenification would be an unlikely presentation. An id reaction responds to treatment of the underlying cause.4
Pustular psoriasis is a rare form of the autoimmune disease psoriasis, characterized by white pustules surrounded by erythematous skin. It can be generalized or focal, and has a cyclic nature with reddening of the skin followed by pustule eruption.5
| Condition | Characteristics |
|---|---|
| Id reaction | Intensely pruritic, symmetric, maculopapular or papulovesicular rash; can have widespread follicular pustules |
| Kerion | Raised, spongy lesion that is painful and sometimes indurated; typically associated with tinea capitis |
| Pustular psoriasis | White pustules surrounded by erythematous skin; autoimmune etiology |
| Staphylococcal abscess | Area of redness and induration with painful fluctuance; associated with fever and other systemic symptoms |
