Apophysitis and osteochondrosis are common causes of pain in growing bones but have differing etiologies and required management. Apophysitis results from a traction injury to the cartilage and bony attachment of tendons in children and adolescents. Most often it is an overuse injury in children who are growing and have tight or inflexible muscle tendon units. Although apophysitis occurs in upper and lower extremities, it occurs more often in the lower extremities, with common locations including the patellar tendon attachment at the patella or tibia (i.e., Larsen-Johansson and Osgood-Schlatter diseases), the calcaneus (i.e., Sever disease), and multiple locations around the hip, including the anterior inferior iliac spine. Other locations include the medial epicondyle, which is common in patients who throw or participate in racket sports, and more rarely at the base of the fifth metatarsal (i.e., Iselin disease). Radiography can be helpful in evaluating for other pathologies but is usually not necessary. Treatment includes stretching the affected muscle groups, relative rest, offloading the affected tendon, icing after activity, and limited use of nonsteroidal anti-inflammatory drugs. Osteochondrosis presents less commonly and refers to degenerative changes in the epiphyseal ossification centers of growing bones. Unlike apophysitis, the etiology of osteochondrosis is unknown. Multiple possible etiologies have been explored, including genetic causes, hormonal imbalances, mechanical factors, repetitive trauma, and vascular abnormalities. Other locations of osteochondrosis include the second metatarsal head (i.e., Freiberg disease), the navicular bone (i.e., Köhler bone disease), the femoral head (i.e., Legg-Calvé-Perthes disease), and the capitellum (i.e., Panner disease). Radiography results may be normal initially; magnetic resonance imaging is more sensitive to early changes. Osteochondrosis generally resolves with relative rest, but close monitoring is needed to ensure resolution. Surgery is rarely needed for either apophysitis or osteochondrosis.
Apophysitis results from a traction injury to the cartilage and bony attachment of tendons in children. Most often it is an overuse injury in growing children, especially those with tight or inflexible muscle tendon units. Osteochondrosis presents less commonly and refers to degenerative changes in the epiphyseal ossification centers of growing bones. Unlike apophysitis, the etiology of osteochondrosis is unknown. The most well-known form of osteochondrosis is Legg-Calvé-Perthes disease. The term osteochondrosis is often confused with the term apophysitis; however, these two conditions should be considered separately because they have different etiologies and management. Table 1 provides a summary of apophysitis and osteochondrosis disorders.1
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | Comments |
|---|---|---|
| Preventive measures for medial epicondyle apophysitis should include taking at least four months off from competitive pitching per year, avoiding use of radar guns, and avoiding the combination of pitching and catching.18,19 | C | Major League Baseball position statement for adolescent baseball pitchers |
| Treatment of Osgood-Schlatter disease should include relative rest and quadriceps and hamstring stretching and strengthening.4,9,16 | C | Based on expert opinion and consensus guidelines in the absence of clinical trials |
| Sever disease treatment should include relative rest, heel cups initially, and heel cord stretches to prevent recurrence.23–25 | B | Based on a small randomized controlled trial |
| Osteochondrosis disorders are rare and many are self-limiting. However, physicians should have a low threshold to refer to a pediatric orthopedist, especially if the condition persists longer than four to six months.27,30,31 | C | Based on expert opinion and consensus guidelines in the absence of clinical trials |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
TABLE 1 Summary of Apophysitis and Osteochondrosis Disorders
| Disorder | Clinical presentation | Radiographic findings | Initial treatment | Orthopedic referral |
|---|---|---|---|---|
| Apophysitis | ||||
| Hip apophysitis | Pain over affected apophysis (seven sites in pelvis) | Normal or widened apophysis compared with contralateral side | Rest from painful sport or activities | Patients with persistent pain despite conservative management |
| Iselin disease | Insidious onset of pain over base of fifth metatarsal head | Normal or widened apophysis of the proximal metatarsal | Rest, stiff-soled shoe for protected weight-bearing | Patients with acute avulsions or continued symptoms despite rest |
| Larsen-Johansson disease | Pain at inferior patellar pole with activity and kneeling | Soft tissue swelling and calcification of inferior pole of patella | Activity modification; short course of acetaminophen or NSAIDs | Patients with a mature skeleton who have persistent symptoms |
| Medial epicondyle apophysitis (i.e., thrower's elbow) | Localized pain over medial epicondyle with throwing | May show fragmentation or widening of medial epicondyle | Throwing cessation; acetaminophen or NSAIDs as needed | Patients with acute avulsions or continued symptoms despite rest |
| Osgood-Schlatter disease | Pain at anterior tibial tubercle with activity and kneeling | Soft tissue swelling and fragmentation of tibial tubercle | Activity modification; acetaminophen or NSAIDs | Patients with a mature skeleton who have persistent symptoms |
| Sever disease | Posterior heel pain with activity and shoe wear | Plain radiography results are usually normal | Activity and shoe modifications; heel cups; calf stretches; acetaminophen or NSAIDs | Patients with a mature skeleton who have persistent symptoms |
| Osteochondrosis | ||||
| Freiberg disease | Metatarsal head pain and swelling | Sclerosis, flattening and fragmentation of metatarsal head | Activity modification; metatarsal pads; well-padded shoes; limited NSAIDs for pain | Patients with metatarsophalangeal joint arthritis and loose joint fragments |
| Köhler bone disease | Midfoot pain and limp | Sclerosis, flattening, and fragmentation of navicular bone | Cast immobilization for up to four to six weeks | Patients with recent trauma, illness, or elevated inflammatory markers |
| Legg-Calvé-Perthes disease | Pain in hip, limping child, possible referred knee pain | Sclerosis, flattening and fragmentation of the femoral head | No weight-bearing activities (e.g., sports, dance) until reossification | Patients with a confirmed or suspected diagnosis |
| Panner disease | Vague, lateral-sided elbow pain | Flattening and fragmentation of humeral capitellum | Rest; acetaminophen or NSAIDs | Patients with loose joint fragments |
NSAIDs = nonsteroidal anti-inflammatory drugs.
Adapted with permission from Atanda A Jr., Shah SA, O'Brien K. Osteochondrosis: common causes of pain in growing bones. Am Fam Physician. 2011;83(3):290.
Apophysitis
Approximately one-third of school-aged children visit a health care professional each year for a sports injury.2 Apophysitis is responsible for a large percentage of these visits.3 The age of onset can vary, but apophysitis is notable during episodes of growth when bone lengthening outpaces lengthening of associated muscle tendon units.4 Surgery is rarely needed for apophysitis.
PATHOPHYSIOLOGY
The apophysis is two to five times weaker than the surrounding structures, including the muscle tendon complex, ligaments, and bones.5 Inflexibility as well as bone growth before muscle lengthening can contribute to increased tension at the apophysis.4 Certain sports and activities have a predilection for specific apophyseal locations. Running sports can affect the hips, knees, and ankles, whereas overhead sports can affect the shoulders, elbows, and wrists.
DIAGNOSIS
The typical clinical diagnosis of apophysitis is based on history and examination.5 Examination findings include localized swelling and pain at the apophysis that worsen with resisted activation of the associated muscle tendon complex.6 Radiography can be performed to demonstrate the severity of the injury and help evaluate for other possible causes such as avulsion, stress fractures, fragmentation of the ossification center, and even malignancy.5 Office-based ultrasonography is user dependent but can show a widened and fragmented apophysis and provide contralateral comparison.7 Ultrasonography has no radiation risk, is more sensitive than plain radiography, and can confirm the absence of a muscle and tendon injury.7
TREATMENT
The mainstay for treatment of apophysitis is stretching and relative rest while maintaining activities as tolerated. Other options for symptom treatment include icing and limited use of oral or topical nonsteroidal anti-inflammatory drugs (NSAIDs). Apophysitis is a self-limiting disorder that resolves by improving the patient's flexibility or when the patient stops growing and the apophyseal centers fuse.8,9 Most patients do well with conservative therapy, and only a small minority require surgical intervention.9 Rest from the overuse activity and cross-training with biking or swimming can also be helpful.
PREVENTION
Prevention of overuse conditions can be accomplished by reducing early sports specialization (before high school) and overtraining.10 Patients undergoing growth spurts are especially vulnerable as bone growth outpaces muscle lengthening, adding to inflexibility of the joint. Promoting engagement in a variety of sports or cross-training activities may be beneficial.10
COMMON DISORDERS AND DISEASES
Hip Apophysitis. There are seven apophyseal locations in the developing pelvis11 (Figure 1). The anterosuperior and anteroinferior iliac spines (i.e., sartorius and rectus femoris origins, respectively), the iliac crest, and the ischial tuberosity (i.e., hamstring) are at risk of injury in running, kicking sports, and dancing.12 Injuries can result from acute avulsion (Figure 2A), blunt trauma, or chronic traction13 (Figure 2B). Pain localized at a tendinous insertion should prompt further evaluation for the disorder. Initial radiography may show avulsion of the apophysis or be normal. Office-based point-of-care ultrasonography is a useful imaging modality. Draping should be required, and a parent or assistant should be present. Ultrasonography can demonstrate tenderness via sonopalpation and a widened or fragmented apophysis compared with the contralateral side.13 Treatment includes relative rest and stretching of the hip flexors or quadriceps and the hamstring complex, with a gradual return to pain-free activity, often within several weeks to months.8
FIGURE 1
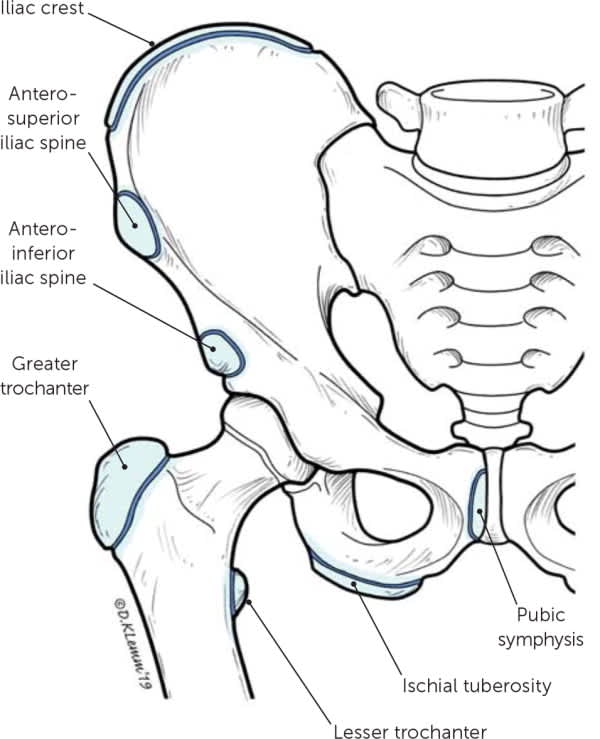
Locations of hip apophysitis.
Illustration by Dave Klemm
FIGURE 2

Apophysitis of the hip. (A) Acute mildly displaced avulsion fracture of the left anterosuperior iliac spine apophysis (arrow). Treatment was conservative, and the patient recovered within two months. (B) Sonogram showing widening of the apophysis (arrow) in a patient with chronic traction apophysitis.
Iselin Disease. Iselin disease is a traction injury of the peroneus brevis on the apophysis at the base of the fifth metatarsal. It affects boys at a younger age than girls and is caused by repetitive microtrauma of the peroneus brevis on the apophysis or a history of inversion injuries.14 This should not be confused with avulsion fractures, which are the result of an acute injury. Examination findings include pain and swelling at the base of the fifth metatarsal and pain and discomfort with resisted eversion, passive inversion, or plantar flexion.14 Radiographic results can be normal (Figure 3A) or show fragmentation and widening of the apophysis at the medial epicondyle.14 Magnetic resonance imaging (MRI) may be indicated if severe symptoms persist to confirm that the symptoms are not caused by a stress fracture (Figure 3B). Treatment includes relative rest with a stiff-soled or postoperative shoe for severe pain.14
FIGURE 3

Iselin disease. (A) Plain radiograph, oblique view showing a normal-appearing apophysis. (B) Magnetic resonance imaging showing edema at the fifth metatarsal base with adjacent edema consistent with apophysitis.
Larsen-Johansson Disease. Larsen-Johansson disease (i.e., patellar apophysitis) is a traction injury of the inferior pole of the patella. Patients present with anterior knee pain that is irritated by jumping. Larsen-Johansson disease is most common in athletic children and adolescents between the ages of 10 and 12.15 Tenderness with palpatation is most acute at the lower pole of the patella.13 Radiography can show an abnormal calcification of ossification centers, whereas ultrasonography may show further fragmentation of the inferior patella16 (Figure 4A). Plain radiography can help confirm the absence of a patellar sleeve avulsion (Figure 4B). Treatment options include a short course of NSAIDs or acetaminophen; icing; patellar counterforce strap; hamstring, quadriceps, and heel cord stretches; and relative rest.16 It can take 12 to 24 months for symptoms to completely resolve. It is unusual for pain to persist after fusion of the apophysis.16
FIGURE 4

Larsen-Johansson disease. (A) Minimal fragmentation at inferior patellar pole. (B) Knee radiograph showing subacute patellar sleeve fracture.
Medial Epicondyle Apophysitis. Thrower's elbow (i.e., Little Leaguer's elbow) is a common overuse disorder in throwing athletes, especially in those who play baseball (20% to 40% of school-aged pitchers).17 It is a traction injury at the location of the medial epicondyle physeal plate.17 Risk factors include high pitch counts per game, pitching on multiple teams, coach-driven incentives to pitch harder, radar gun usage to measure speed, and not taking enough time off from the sport during the year.18 Major League Baseball and USA Baseball provide Pitch Smart guidelines that support at least a four-month rest from competitive pitching per year for prevention of this disorder, as well as avoiding playing both catcher and pitcher on the same team.19 Examination findings include tenderness with palpation on the medial epicondyle or resisted flexion/pronation with valgus stress or the “milking maneuver”18 (Figure 5; https://www.youtube.com/watch?v=SwigwaZxBXEamp;&t=10s).
FIGURE 5

Milking maneuver.
Treatment calls for refraining from overhead throwing, limited NSAID use, strengthening of the scapular retractors, and a gradual return to activities when the patient is free of pain. Rehabilitation programs for throwers such as Advanced Thrower's Ten can also be considered (http://www.kevinwilk.com/assets/advancedthrowers10-7-22-16.pdf).20 Because of high recurrence rates, avoidance of common throwing positions such as pitching and catching should be considered for up to one year or until after fusion of the apophysis.18 Immobilization and surgery are rarely required and are indicated only for refractory cases or for patients with significant avulsion fractures.8,21
Osgood-Schlatter Disease. Osgood-Schlatter disease is a traction injury of the insertion of the patellar tendon to the tibial tubercle. Prevalent during growth spurts, it is more common in athletes vs. nonathletes (21% vs. 4.5%, respectively).22 Pain is noted over the tibial tuberosity when going down stairs, jumping, or applying direct pressure when kneeling.6 It is bilateral in 30% of cases.9 Physicians may note swelling over the tibial tuberosity with associated tenderness to palpation. Quadriceps and hamstring tightness are commonly associated with this disease.22 Radiography is usually not needed but can help the physician assess for a tibial stress fracture or avulsion fracture of the tibial tubercle, especially if tenderness is significant and weight-bearing is difficult (Figure 6). Ultrasonography can show swelling and fragmentation of the tibial tubercle and increased blood flow over the apophysis.4 Treatment includes relative rest, exercise programs designed to increase flexibility and strengthen the quadriceps and hamstrings, and use of acetaminophen or NSAIDs.6 School-aged children should be encouraged to participate in sports and activities as tolerated given the benign nature of the disease.9
FIGURE 6

Osgood-Schlatter disease (apophysitis of the tibial tubercle).
Sever Disease. Sever disease (i.e., calcaneal apophysitis) is the most common cause of heel pain in children and adolescents.23 It occurs at the point of insertion of the Achilles tendon to the calcaneus and is often aggravated by running or jumping.24 The incidence ranges from 2% to 16% in children.24,25 Onset is gradual and most common in eight- to 12-year-old children.26 Risk factors include a tight heel cord, running or jumping sports, and early sport specialization.26 Examination findings include tenderness at the heel when squeezed (Figure 7A). Calcaneal radiographic results are usually negative (Figure 7B) but can be used to evaluate for rare stress fractures.5 Initial treatment includes icing, heel cups, and heel cord stretching, and treatment with acetaminophen or NSAIDs.24 Patients can participate in pain-free activities only as they recover.24
FIGURE 7

Sever disease. (A) Squeeze test. (B) Radiograph of same patient with normal calcaneal apophysis.
Osteochondrosis
Unlike apophysitis, osteochondrosis is caused by a temporary disruption of the blood supply at the bone-cartilage complex of a particular joint, and not by traction. These diseases are rare, and the etiology of the disruption is unknown. Multiple possible etiologies have been explored, including genetic causes, hormonal imbalances, mechanical factors, repetitive trauma, and vascular abnormalities. Generally, this is a transient disorder that resolves spontaneously but needs close monitoring to ensure resolution. Surgery is rarely needed for osteochondrosis.
FREIBERG DISEASE
Freiberg disease is an idiopathic avascular necrosis of the second digit of the metatarsal head, but it can affect the lesser toes as well.27 It occurs in females more often than males in a 5:1 ratio with dominant foot involvement only 36% of the time.28 The etiology is attributed to microtrauma, impaired vascularity, and systemic disorders.28 Progressive pain localized to the metatarsal head that worsens with walking should raise concern for this disease.27 Initial imaging should include a weight-bearing foot radiography series with findings showing deformation, sclerosis, or flattening of the metatarsal head.27 Radiographic evidence may be delayed three to six weeks from symptom onset, so repeat imaging may be necessary.27 MRI can detect the disease in its earliest stages.27 Initial management includes NSAIDs and protected weight-bearing with a stiff-soled shoe or walking boot. Metatarsal pads can offload the affected site.28 Surgical intervention is reserved for loose bodies and significantly deformed metatarsal heads.27,28
KÖHLER BONE DISEASE
Köhler bone disease is a rare condition mostly affecting children younger than 10 years. It involves avascular necrosis of the navicular bone.29 Patients present with midfoot tenderness and swelling, as well as an antalgic gait that favors the lateral foot. Radiography can show navicular flattening, sclerosis, and fragmentation.29,30 Treatment options include rest, ice, and immobilization in a walking cast for four to six weeks.29,30 Generally, it resolves in one to three years.30
LEGG-CALVÉ-PERTHES DISEASE
Legg-Calvé-Perthes disease is a spontaneous and idiopathic avascular necrosis of the femoral head. It is a rare but disabling disease affecting 10.8 in 100,000 children in a 5:1 male-to-female ratio.31 Patients are usually affected from ages four to eight years.32 Risk factors include short stature, hyperactivity, lower latitude of birth, obesity, low birth weight, and smoking exposure.32
Symptoms and signs include groin pain, referred knee pain, a limp on the affected side, and internal rotation or shortening of the leg.32 Radiographic findings on anteroposterior and frog-leg lateral views can be delayed early in the course of the disease but can later show flattening or fragmentation of the femoral head.32 MRI findings are variable, but the most common early findings include effusion and changes to the labrum and articular cartilage.32 Treatment includes offloading the joint, and restriction of activities until there is evidence of resolution. Referral to a pediatric orthopedist is indicated because of the risk of long-term sequelae, including permanent deformity of the femoral head.
PANNER DISEASE
Osteochondrosis of the capitellum (i.e., Panner disease) most often affects children younger than 10 years, and more than 90% are boys.33 It is more common in athletes that have repetitive valgus or axial stresses on the elbow, such as baseball and gymnastics, respectively.33 Presentation can vary with lateral elbow pain, stiffness, and limited range of motion. Imaging can include radiography and MRI with findings of irregularity at the capitellum (humerus) and epiphysis.33 Panner disease is self-resolving.33 Treatment entails rest from activities, a four-week period of immobilization, a short course of NSAIDs or acetaminophen for pain, and radiographic monitoring for four to six months.34 This disease should be differentiated from osteochondritis dissecans of the capitulum that involves the articular cartilage, not the epiphysis.17 If uncertain, consider referral to a pediatric orthopedist.17
Orthopedic Referral
Most apophysitis disorders are self-resolving with conservative management. Considerations for sports medicine or orthopedic referral can include pain persisting after fusion of apophyseal sites or cases refractory to conservative management.6 Osteochondrosis disorders are less common and many resolve with a period of relative rest and close monitoring; however, earlier involvement of a pediatric orthopedist would be reasonable if spontaneous resolution of pain does not occur within four to six months.27,32,33
In addition to the above cautions, consideration of and workup for more serious disease may be indicated depending on the presenting symptoms. Appropriate referral is warranted in the presence of any of the following warning signs: severe pain, history of trauma, inability to bear weight, odd location of pain, night pain, systemic signs of illness or infection, or a history of cancer.10 Figure 8 shows common locations of apophysitis and osteochondrosis.1 Although rare, inflammatory arthropathies in children, especially in multiple joints, should be considered, and further evaluation and referral to a pediatric rheumatologist would be warranted.10 Stress fractures should also be considered if no radiographic evidence of osteochondrosis is apparent and the pain does not localize to apophyseal centers.10
FIGURE 8
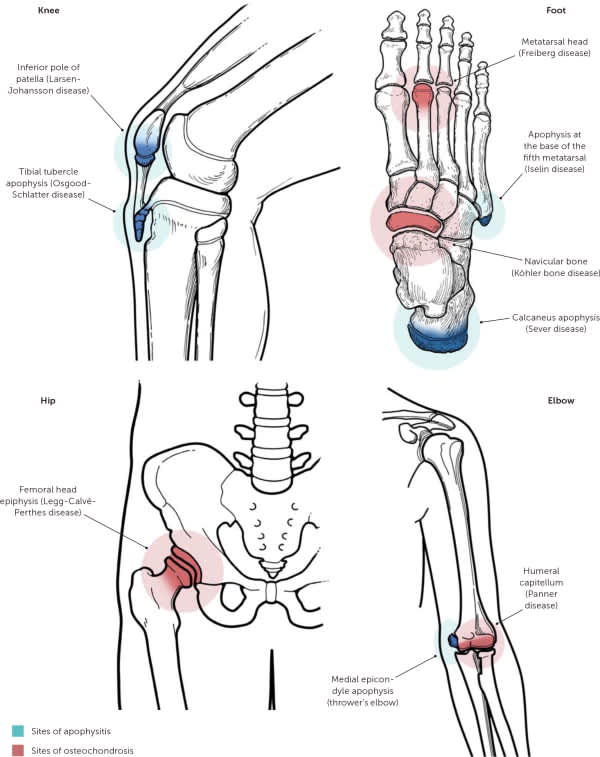
Overview of apophysitis and osteochondrosis locations.
Illustration by Dave Klemm
Adapted with permission from Atanda A Jr., Shah SA, O'Brien K. Osteochondrosis: common causes of pain in growing bones. Am Fam Physician. 2011;83(3):286.
This article updates a previous article on this topic by Atanda, et al.1
Data Sources: A search was completed using the Cochrane Database of Systematic Reviews, Cochrane Central Register of Controlled Trials, National Guideline Clearinghouse, and PubMed. Key words included: apophysitis, osteochondrosis, Sever disease, Osgood-Schlatter disease, Legg-Calvé-Perthes disease, Panner disease, and pediatric joint pain. The search included meta-analyses, systematic reviews, randomized controlled trials, clinical trials, guidelines, and diagnostic studies. Search dates: March to June 2018, and February 2019.
