Newborn male circumcision is a common elective surgical procedure for the removal of foreskin covering the glans penis. The American Academy of Pediatrics, the American College of Obstetricians and Gynecologists, the Centers for Disease Control and Prevention, and the American Academy of Family Physicians recognize that there are health benefits of newborn male circumcision but do not universally recommend the procedure. Performing male circumcision during the neonatal period has several advantages, including a lower risk of complications, faster healing, and lower cost. The three most common techniques for newborn male circumcision utilize the Mogen clamp, the Gomco clamp, or the Plastibell device. Complications are uncommon and can include bleeding, injury to the penis, adhesions, excessive skin removal, phimosis, and meatal stenosis. Anatomic and medical contraindications may require that the procedure be deferred beyond the neonatal period. Infants with anatomic abnormalities should be referred to a pediatric urologist. Physicians should present information about potential benefits and risks rather than withholding or recommending circumcision. Parents should weigh the health benefits and risks and consider their own religious, cultural, and personal preferences when making the decision.
Newborn male circumcision is a common elective surgical procedure for the removal of foreskin covering the glans penis. It is most often performed in the first days of life.1 According to the World Health Organization, there are several advantages of circumcising males at a younger age, including a lower risk of complications, faster healing, and lower cost.2,3 The frequency of adverse events is four per 1,000 procedures for early infant circumcision, but this number increases 10- to 20-fold in older boys.4 Physicians should present information about potential benefits and risks rather than withholding or recommending circumcision, and parents should consider their own religious, cultural, and personal preferences when making the decision.3,5
SORT: KEY RECOMMENDATIONS FOR PRACTICE
| Clinical recommendation | Evidence rating | Comments |
|---|---|---|
| Parents should be offered newborn circumcision in a nonbiased conversation regarding potential benefits and harms.3,6,7 | C | Expert opinion and consensus guidelines |
| The Mogen clamp, the Gomco clamp, and the Plastibell device can be used effectively for newborn circumcision.19 | C | Usual practice and expert opinion in the absence of clinical trials |
| Local anesthesia should be used during newborn circumcision.26–30 | B | Randomized controlled trials and meta-analyses showing benefit |
| Infants with abnormal penile anatomy should be referred to a pediatric urologist for circumcision.1,20,22 | C | Usual practice and expert opinion in the absence of clinical trials |
A = consistent, good-quality patient-oriented evidence; B = inconsistent or limited-quality patient-oriented evidence; C = consensus, disease-oriented evidence, usual practice, expert opinion, or case series. For information about the SORT evidence rating system, go to https://www.aafp.org/afpsort.
The American Academy of Pediatrics (AAP), the American College of Obstetricians and Gynecologists, the Centers for Disease Control and Prevention (CDC), and the American Academy of Family Physicians (AAFP) recognize the potential health benefits of newborn male circumcision, but they do not universally recommend the procedure.3,6,7 The AAFP recommends that circumcision be available and covered by health insurance for those who desire it.7
Established health benefits of circumcision include a reduced lifetime incidence of urinary tract infections, penile cancer, phimosis, HIV, and several other sexually transmitted infections.3,6,8–10 A 2017 systematic review concluded that the health benefits of newborn circumcision are greater than the risks associated with the procedure.11 Despite these benefits, the newborn male circumcision rate has declined in the United States, from 83% in the 1960s to 77% in 2010.12 There are racial and ethnic differences in the overall circumcision rate: over the past decade, 91% of white males reported having been circumcised compared with 76% of black males and 44% of Hispanic males.5,8,11,13 In some states, these differences may be related to an increasing Hispanic population and lack of Medicaid coverage.11 The data used by the AAP and CDC to support their policy statements have largely been extrapolated from adult circumcision studies performed in the sub-Saharan region of Africa. Because of the lack of direct evidence of benefit, some consider newborn circumcision unnecessary.9,14 A 2010 systematic review found that although complications are rare, there is little evidence to support circumcision.15
Embryology and Anatomy
Knowledge of penile embryology and anatomy is imperative before attempting circumcision.16,17 Male development is influenced by the Y chromosome, which begins development of the external genitalia at seven to 17 weeks' gestation.16 The nerve sensation of the penile skin is supplied by the dorsal nerve, which is absent at the 12 o'clock position. The internal pudendal artery is the main blood supply of the penis, and it is drained by the deep dorsal vein. The cavernosal, dorsal, and bulbourethral arteries and veins are the offshoots of these two main vessels. In newborns, prepuce or preputial adhesions between the glans and foreskin are normal.1
Circumcision Techniques
The three most common techniques 18 for circumcision utilize the Mogen clamp (Figure 1), the Gomco clamp (Figure 2), or the Plastibell device (Figure 3). Because these techniques are equally effective, the choice of device should be guided by the physician's experience and comfort level.19,20 The Mogen and Gomco clamps protect the glans, and the Plastibell induces tissue necrosis, which is sloughed off with the plastic shield.21
FIGURE 1.
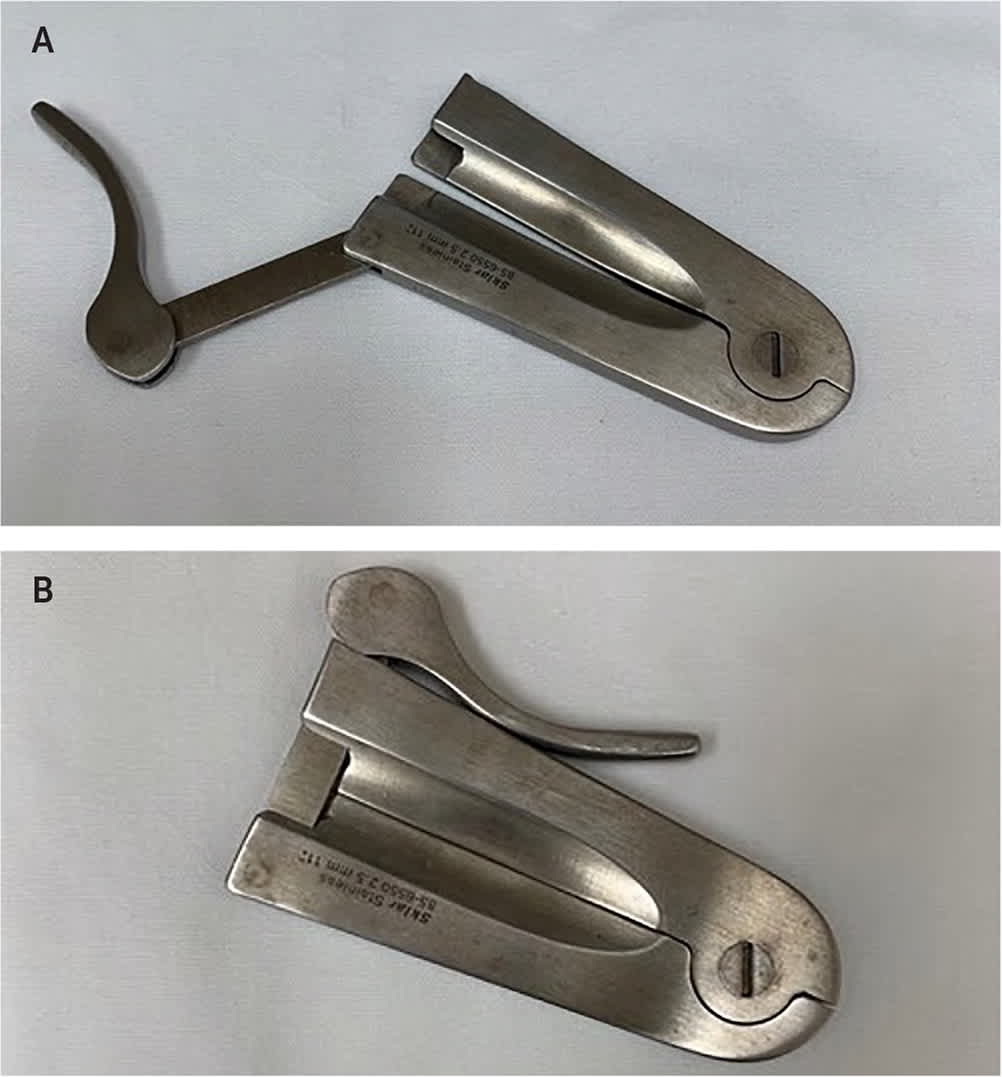
Mogen clamp in the open (A) and closed (B) positions.
FIGURE 2.
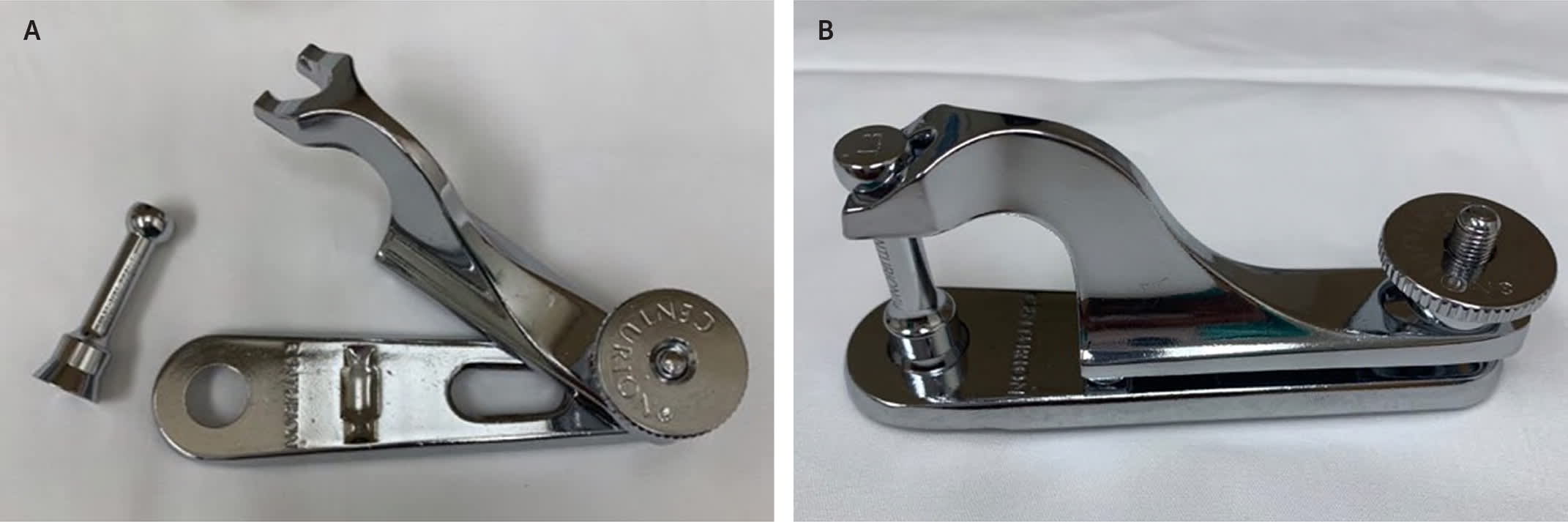
Gomco clamp in the open (A) and closed (B) positions.
FIGURE 3.

Plastibell device.
When using the Gomco clamp or Plastibell, the choice of device size depends on the diameter of the glans rather than penile length.22 The Gomco clamp ranges from 1.1 to 1.6 cm, and the Plastibell from 1.1 to 1.7 cm. The most commonly used size for either device is 1.3 cm.23 Circumcision using the Mogen clamp can be completed in less than five minutes, whereas procedures using the Gomco clamp or Plastibell can take up to 10 minutes.24,25 In general, the time required to complete the procedure is inversely related to the physician's level of experience.
Anesthesia
Anesthesia should be provided to all newborns undergoing circumcision, regardless of the technique.26–30 A randomized trial suggested that procedures using the Mogen clamp produce less pain than those using the Gomco clamp.25 Pain relief can be achieved using lidocaine/prilocaine cream applied to the foreskin 30 to 60 minutes before the procedure. Alternatively, nerve blocks can be performed about five minutes before the procedure using 1% lidocaine without epinephrine: a dorsal penile nerve block requires 0.2- to 0.4-mL injections on either side of the midline at the base of the penis (Figure 4A), and a ring block requires a 0.8-mL injection circumferentially around the base of the penis (Figure 4B). A 2004 Cochrane review found that the ring block or dorsal penile nerve block is more effective than topical lidocaine/prilocaine alone.28 A sucrose pacifier (i.e., sucrose solution squirted in the mouth followed by a pacifier) is another analgesic option.26 A recent randomized controlled trial comparing lidocaine/prilocaine cream alone with combination analgesics (lidocaine/prilocaine plus sucrose; lidocaine/prilocaine plus sucrose plus dorsal penile nerve block; and lidocaine/prilocaine plus sucrose plus ring block) showed that combination analgesics, especially topical anesthetic plus sucrose plus ring block, are more effective.30
FIGURE 4.
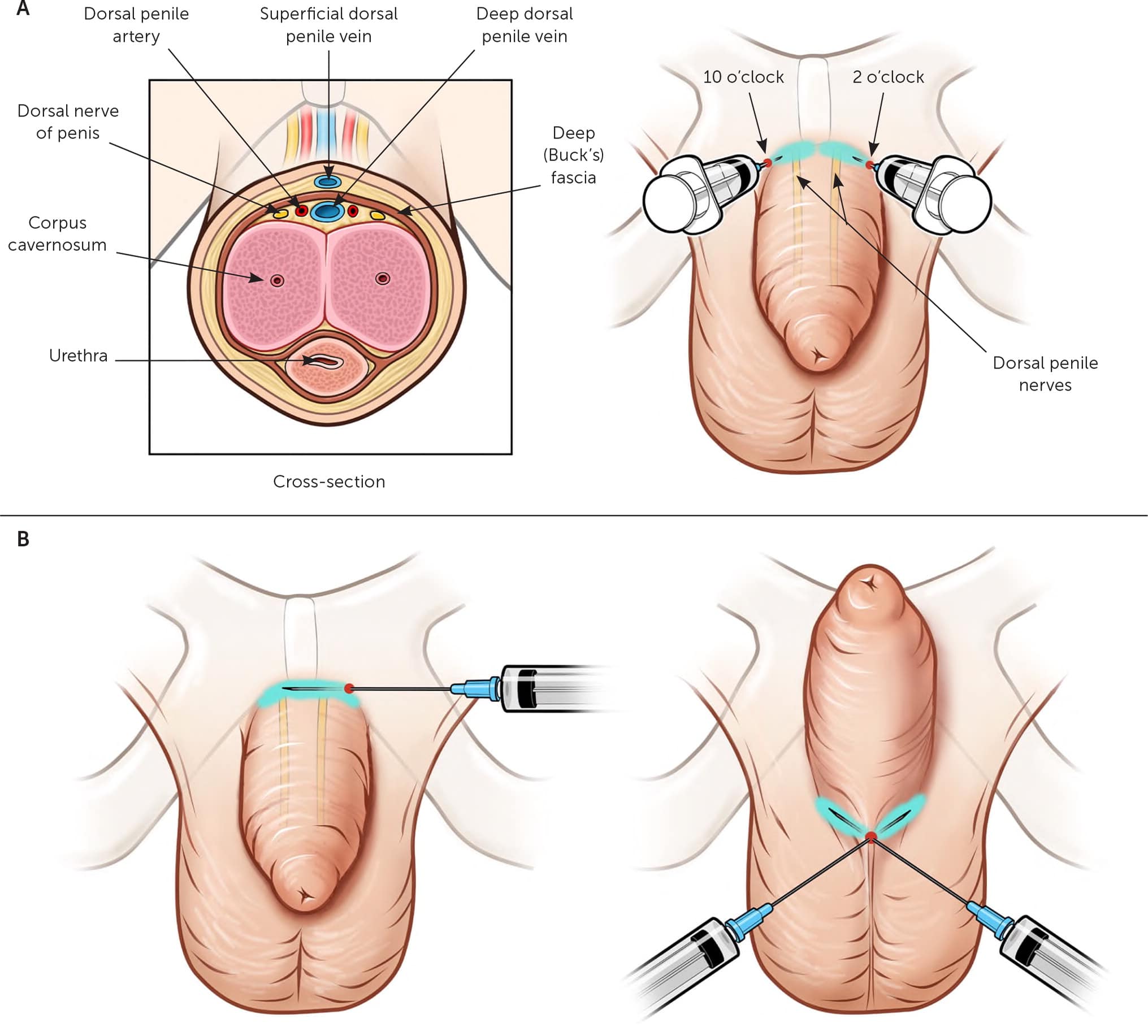
Nerve blocks used for anesthesia during circumcision. (A) Dorsal penile nerve block. With a single syringe, inject 0.2 to 0.4 mL of lidocaine subcutaneously at the base of the penis in the 10 and 2 o'clock positions to anesthetize both branches of the dorsal penile nerve. (B) Ring block. With a single syringe, inject 0.8 mL of lidocaine subcutaneously around the perimeter of the base of the penis. Two or more injections will be needed to complete the circumferential block.
Illustration by Dave Klemm
Procedure
The duration of the procedure, bleeding, and complications vary depending on which device is used. The Mogen clamp requires the least training and procedure time, and it is associated with less bleeding and fewer complications. The Gomco clamp and Plastibell require more training and longer procedures, and are associated with more bleeding and more complications.18,25,31,32
The procedure setup, including the aseptic field, anesthesia, and positioning of the infant, is the same regardless of the device used 21 (Table 122 ). There is little variation in the first few steps once analgesia has been achieved. Straight hemostats are applied to the distal end of the foreskin at the 10 and 2 o'clock positions. A lubricated curved hemostat (pointed away from the penis) is used to lyse the adhesions on the right and left sides of the glans, avoiding the ventral frenulum.20
TABLE 1. Preparation for Newborn Circumcision
| Lidocaine/prilocaine 2.5%/2.5% cream is applied 30 to 60 minutes before the procedure |
| The infant is placed in a supine position and restrained by an assistant or in an infant holder with hook-and-loop fastener straps |
| The penis and scrotum are cleaned with povidone-iodine solution and draped in a sterile fashion |
| Local anesthetic (dorsal penile nerve block or ring block [Figure 4]) is injected before the procedure |
| The distal end of the foreskin is clamped at the 10 and 2 o'clock positions with straight hemostats |
| A lubricated curved hemostat (pointed away from penis) is used to lyse the adhesions on the right and left sides to the base of the glans penis, avoiding the ventral frenulum |
Information from reference 22.
GOMCO CLAMP
A video demonstrating a circumcision using a Gomco clamp is available. For this technique, a straight hemostat is applied at the 12 o'clock position to create a crush line. With blunt-edge scissors facing the glans, a small incision is made one-third to one-half the distance from the coronal margin to expose the glans. The foreskin is retracted to break away any remaining adhesions. The bell of the clamp is placed under the foreskin and over the glans, and the foreskin is pulled over the bell with the attached hemostats. A hemostat or a small safety pin is used to bring the edges of the dorsal incision together over the flare of the bell before the base plate is applied. The hemostats at the 10 and 2 o'clock positions are removed, the foreskin is gently pulled through the hole in the base plate, and the base plate is placed over the bell. The tip of the incision should be visible above the base plate. The yoke of the top plate (rocker arm) is attached to the arms of the bell, and the other end of the top plate is tightened to the base plate and left in place for five minutes. During this time, excess foreskin is removed with a scalpel. After five minutes, the plates are loosened and the clamp disassembled, and sterile gauze is used to gently tease the crushed foreskin off of the bell.
MOGEN CLAMP
See a video demonstrating a circumcision using a Mogen clamp. Once the adhesions have been lysed, the glans is pushed downward. The foreskin is held with hemostats at the 9 and 3 o'clock positions, then slid between the narrowly opened (3 mm) Mogen clamp. The clamp is applied with the concave surface facing downward after ensuring that the distal glans (tip of the penis) is not caught in the clamp. The clamp is closed and left on for 60 to 90 seconds. Excess foreskin is removed with a scalpel, then the clamp is removed. Starting at either end to avoid injuring the urethra, the probe is used to gently separate the foreskin, then push it down below the corona, fully exposing the glans and breaking away any remaining adhesions.
PLASTIBELL
The Plastibell technique begins similarly to the Gomco clamp technique. A straight hemostat is applied at the 12 o'clock position to create a crush line, then with blunt-edge scissors facing the glans, a small incision is made one-third to one-half the distance from the coronal margin to expose the glans.33 The foreskin is retracted to break away any remaining adhesions. The Plastibell is placed under the foreskin and over the glans, then the foreskin is pulled over the Plastibell and stabilized by clamping it to the handle of the Plastibell with hemostats. The Plastibell is secured in place by tying a string around the groove on the bell, then excess foreskin past the outer edge is removed with a scalpel and the handle is broken off, leaving the ring in place.
Postprocedure Care
Petroleum jelly and gauze are applied to the glans after the procedure to keep the diaper from sticking to the wound during the healing period. The newborn can be discharged from the hospital after the procedure; it is not necessary to wait until he urinates. The parents are usually advised to follow up in three to five days and should be counseled on applying the dressing with each diaper change until healing is complete or until the Plastibell falls off. This usually takes five to seven days.21,34
Complications
The frequency of adverse events is four per 1,000 for early infant circumcision and 10- to 20-fold higher in older boys, according to a 2014 study assessing adverse outcome rates by age at circumcision.4 Minor bleeding is the most common early complication.20 Infants who are vitamin K deficient may have prolonged bleeding. Postprocedure bleeding commonly occurs during the first week of life, but it can occur for up to eight weeks.
Glans injury can occur with all three techniques, and insufficient or excessive skin removal can occur with the Mogen and Gomco clamps.20 Meatal stenosis is the most common late complication and is usually prevented by advising parents to apply petroleum jelly to the glans.35
More serious and late complications include penile injury or amputation, infection, necrosis of the glans, incision of the glans or urethra, adhesions, phimosis, and meatal stenosis and scarring. Infants with these conditions should be referred to a pediatric urologist.3,4,7,20,32,36
Contraindications
There are anatomic and medical contraindications to newborn circumcision (Table 2).1 In some cases, an anatomic variant may not be noticed until after the procedure has begun and the foreskin retracted.1,17,22 Newborns with abnormal penile anatomy should be referred to a pediatric urologist for appropriate care.20,22
TABLE 2. Contraindications to Newborn Circumcision
| Anatomic contraindications Chordee Concealed penis Congenital megaprepuce Epispadias Hypospadias Penile torsion Penoscrotal webbing |
| Medical contraindications Admission to neonatal intensive care unit Age < 12 hours Bleeding dyscrasias (e.g., hemophilia) Current illness Jaundice |
Information from reference 1.
This article updates a previous article on this topic by Peleg and Steiner.22
Data Sources: A PubMed search was completed using the key terms newborn circumcision, Mogen clamp, Gomco clamp and Plastibell, anesthesia and circumcision, and treatment options. The search included meta-analyses, randomized controlled trials, clinical trials, and reviews. We also searched the Cochrane database and Essential Evidence Plus. References in these resources were also searched. Search dates: November 2018 to March 2020.
